
![]()
При посиланні на статтю з нашого журналу
необхідно вказувати:
- назву журналу
українською мовою - Медичні перспективи
або транслітерацією - Medicni perspektivi
- DOI статті
![]()


Key words: tennis, athlete, nutrition, performance
Ключові слова: теніс, спортсмен, харчування, продуктивність
Abstract
Nutrition is crucial in improving athlete performance, and research on the relationship between nutrition and sport continues to grow. This article aims to investigate nutrition's influence on tennis athletes' performance through a systematic review approach. The main objective was to identify the types of food that are most influential in improving the performance of tennis athletes, as well as to evaluate their impact on physiological and psychological aspects. This study used a systematic review approach, following PRISMA guidelines. Databases such as PubMed, Scopus, and Web of Science were reviewed for articles published up to 2024, using keywords related to nutrition and tennis. Inclusion and exclusion criteria were set to select articles that fit the research topic. Data were then extracted, synthesized, and analyzed to produce significant findings in the context of nutrition's influence on tennis athletes' performance. Of the 500 articles identified, 44 met the inclusion criteria. The analysis concluded that nutrition is essential in enhancing a tennis athlete's performance. Carbohydrates, protein, and fat were shown to be vital sources of energy for tennis athletes, while vitamins and minerals play an essential role in recovery and optimal body function. Previous studies have also shown that proper diet and supplementation can significantly improve tennis athletes' stamina, strength, and recovery. This study confirms that proper nutrition is highly influential in improving the performance of tennis athletes. Optimizing carbohydrate, protein, fat, vitamin, and mineral intake can have significant physiological and psychological benefits such as stamina, strength, and recovery. These findings result in recommendations for a tennis athlete's diet tailored to individual needs. At the same time, further research is recommended to deepen the understanding of the relationship between nutrition and sports performance.
Реферат
Вплив харчування на результативність тенісистів: систематичний огляд. Саюти Йогі, Сабіллах Мухамад Іхсан, Хідаят Резга Аржан, Шоліхах Іма Фітрі. Харчування відіграє вирішальну роль у підвищенні спортивної результативності спортсменів, й інтерес до вивчення взаємозв’язку між харчуванням і спортивними досягненнями продовжує зростати. Метою цієї статті є дослідити вплив харчування на результативність тенісистів за допомогою методу систематичного огляду. Основним завданням є визначення типів харчування, які мають найбільший вплив на спортивні показники, а також оцінювання їхнього впливу на фізіологічні та психологічні аспекти підготовки тенісистів. Дослідження проведено відповідно до методології PRISMA. Було проаналізовано наукові бази даних, зокрема PubMed, Scopus і Web of Science, з використанням ключових слів, пов’язаних із харчуванням і тенісом, для виявлення публікацій до 2024 року. Встановлено чіткі критерії включення та виключення для відбору релевантних статей. Відібрані дані були систематизовані, синтезовані та проаналізовані з метою формулювання обґрунтованих висновків щодо впливу харчування на спортивні результати. З 500 проаналізованих публікацій 44 відповідали критеріям включення. Результати аналізу підтверджують, що харчування має суттєвий вплив на спортивну результативність тенісистів. Встановлено, що вуглеводи, білки та жири є ключовими джерелами енергії, а вітаміни й мінерали відіграють важливу роль у відновленні та підтримці оптимального функціонування організму. Попередні дослідження також засвідчили, що збалансоване харчування і відповідні добавки значно покращують витривалість, силу та процес відновлення. Таким чином, результати цього огляду підтверджують важливість правильного харчування для підвищення спортивної ефективності тенісистів. Оптимізація споживання макро- й мікроелементів може забезпечити значні фізіологічні та психологічні переваги. На основі отриманих даних сформульовано рекомендації щодо розробки індивідуальних програм харчування для тенісистів. У майбутньому доцільно проводити додаткові дослідження з метою глибшого вивчення впливу харчування на спортивні досягнення.
Nutrition is one of the critical factors that influence athletic performance. A proper diet is vital, particularly in competitive sports such as tennis, where energy and recovery requirements are high. Tennis requires a combination of strength, endurance, speed, and agility, thus requiring comprehensive nutritional support to support all these physical aspects [1]. Proper dietary choices increase energy during play, speed up recovery, reduce the risk of injury, and maximize physiological function during matches that last several hours. Correspondingly, research in sports nutrition continues to grow, focusing on how nutrition can be optimized to support athlete performance. Studies have shown that a balanced intake of carbohydrates, protein, and fat is essential in supporting intense and prolonged physical activities, such as those often encountered in tennis [2]. Further research also indicates the importance of micronutrients, such as vitamins and minerals, which are crucial in maintaining athlete health and optimizing performance [3].
This systematic review investigates and analyzes the literature on nutrition's influence on tennis athlete performance. Through in-depth analysis, it aims to identify the nutritional components that are most influential in improving performance and provide recommendations that athletes and coaches can use in designing effective dietary programs. This review will answer the following research questions: What types of nutrition are most effective in improving the performance of tennis athletes, and how do they affect athletes' physiological and psychological aspects during competition? This review hopes to fill a gap in the literature by systematically collecting and synthesizing existing data, which will provide evidence-based guidance in sports nutrition, particularly tennis. According to [4], adequate carbohydrate intake before and during tennis play can significantly improve performance, reduce fatigue, and increase concentration during play. Research [5] supports these findings, stating that protein is crucial for post-match muscle recovery and muscle protein synthesis during high-intensity exercise. This unity in the literature suggests that a combination of carbohydrates and protein is key in the diet of tennis athletes.
Therefore, through this systematic review, we will delve deeper into nutrition's influence on tennis athletes' performance, hoping to provide new insights and valuable global recommendations for the tennis community. With a better understanding of the relationship between nutrition and performance, athletes and coaches can be better guided in setting more effective and efficient nutritional strategies to achieve optimal results on the court.
Review of Nutrition in Sport
1. Carbohydrate, Protein, and Fat in Athletic Nutrition
Carbohydrates, protein, and fat are three macronutrients crucial in supporting athletic performance, including tennis. Carbohydrates are the primary energy source for the body and brain. At the same time, protein plays a role in building and repairing muscle tissue, and fat provides long-term energy and supports complex bodily functions. The importance of each of these macronutrients in supporting the performance of tennis athletes has been widely reviewed in the scientific literature. In tennis, carbohydrates are vital as energy is essential for maintaining athlete performance during long matches. A study published in research [6] stated that adequate carbohydrate intake can improve athlete endurance, slow the onset of fatigue, and support recovery after training or matches. Thus, tennis athletes must ensure the proper carbohydrate intake before, during, and after training or matches to maintain optimal performance. In addition to carbohydrates, protein also plays a vital role in supporting the performance of tennis athletes. Protein is required to repair and build muscle tissue damaged by training or matches and maintain optimal muscle strength and mass. A study found that adequate protein consumption, especially after training, can increase muscle protein synthesis and accelerate muscle recovery.
Therefore, tennis athletes must be mindful of their protein intake to support recovery and maximize muscle adaptation. Fat is also essential to a tennis athlete's diet, although it often receives a negative stigma associated with an increased risk of cardiovascular disease. However, fat is a necessary source of energy, especially for long-duration activities such as tennis matches that last up to several hours. A study [7] showed that fat can be an efficient energy source, especially in low to moderate-intensity activities. Therefore, tennis athletes must focus on healthy fat intake, especially from monounsaturated and polyunsaturated fat sources, to support their stamina and performance during matches. Overall, carbohydrates, protein, and fat are essential components in a tennis athlete's diet that support energy, muscle recovery, and optimal performance. Therefore, tennis athletes must pay close attention to their nutritional intake and ensure they get adequate macronutrients to reach their maximum potential.
2. Essential Vitamins and Minerals
Vitamins and minerals support optimal body function, especially in intense physical activities like tennis. Adequate nutrition can help maintain electrolyte balance, improve muscle recovery, and support the athlete's immune system. In sports, the right balance of vitamins and minerals can significantly affect an athlete's performance. Research has highlighted the importance of vitamins and minerals in sports. For example, a study by [8] states that vitamins and minerals play an essential role in forming enzymes involved in energy metabolism and supporting the immune system. This suggests that vitamins and minerals serve as cofactors in various metabolic processes and play a role in maintaining overall health.
In addition, studies have also shown a correlation between vitamin and mineral intake and athletic fitness. A study conducted by [9] found that athletes with adequate intake of vitamins and minerals tend to perform better and have faster recovery after training or competition [10]. It is confirmed that proper vitamins and minerals can support athletes' stamina and recovery, being essential in tennis, which requires high physical endurance. In addition to supporting physical aspects, vitamins and minerals also have a role in maintaining athletes' mental balance. A study by [11] found that specific vitamin and mineral deficiencies can contribute to decreased mood and concentration, affecting an athlete's overall performance [12]. Proper nutrition can help maintain athletes' mental balance, which is essential in competitive sports such as tennis.
However, it is essential to remember that an excess or deficiency of vitamins and minerals can also negatively impact athletes' health and performance. A study by [13] found that an excess or deficiency of specific vitamins and minerals can lead to health problems such as fatigue, reduced performance, and even injury in athletes. Therefore, it is essential to ensure a balanced and appropriate intake of nutrients according to individual needs. In addition, factors such as the environment and an individual's diet can also affect the nutritional status of athletes. A study conducted [14] concluded that factors such as diet, living habits, and environment can affect athletes' vitamin and mineral intake, making it essential to pay attention to these factors in planning athletes' diets [15]. Besides varying nutritional requirements, external factors must be considered when planning an athlete's diet.
Overall, vitamins and minerals play an essential role in supporting the performance and health of athletes, including tennis athletes. Adequate intake of these nutrients can help improve athletes' stamina, recovery, and mental balance. However, paying attention to individual needs and external factors in planning an athlete's diet to achieve optimal results is essential.
Previous Studies on Nutrition and Tennis
Previous research has revealed the significant impact of diet and supplementation on tennis athletes' performance. Through analyses of specific diets and supplement use, these studies highlight the relationship between nutrition and critical aspects of performance, such as stamina, strength, and recovery. With a focus on practical implications, the studies provide valuable insights into understanding how nutrition affects the overall performance of tennis athletes. Previous studies have examined the relationship between diet and tennis athlete performance. These studies considered general nutrient intakes and specialized diets, such as high-protein or low-carbohydrate diets. A study [16] concluded that a protein-rich diet can improve muscle recovery and strength, which is essential for tennis athletes who experience heavy loading in training and matches. A high-protein diet can also help maintain muscle mass and improve performance [17].
Aside from diet, supplementation has also been the focus of research to improve the performance of tennis athletes. Clinical studies suggest that creatine supplements, which are often used in power sports, may benefit tennis athletes by improving muscle strength and endurance. A study [18] mentioned that creatine can increase training volume and accelerate recovery after strenuous activity.
The importance of electrolytes and hydration has also been a significant research topic in tennis. Loss of electrolytes through sweat during a match can disrupt the ion balance in the body and affect the athlete's performance. In a study conducted [19], it was suggested that electrolyte drinks could help replace lost electrolytes and maintain hydration, thus improving the performance of tennis athletes during long matches. Protein supplements have also been the focus of significant research in the context of post-workout recovery. Athletes often use protein shakes to accelerate muscle recovery after intense exercise. A study by [20] found that consuming protein supplements after exercise can increase muscle protein synthesis and accelerate muscle recovery, thus allowing athletes to recover faster and return to training or matches better.
In addition to improving performance, nutrition also plays a role in reducing the risk of injury in tennis athletes. Diets rich in antioxidants, such as vitamins C and E, have been associated with reduced inflammation and cell damage, which may help prevent athlete injuries. A study by [21] showed that antioxidant supplements may reduce the risk of injury in athletes by reducing levels of inflammation and oxidative stress in the body. Nevertheless, it is also essential to consider the potential side effects of supplementation in athletes. Several studies have highlighted the risks associated with long-term supplement consumption, including digestive problems, kidney damage, and nutritional imbalances [22]. They concluded that a better understanding of the potential risks and benefits of supplementation is needed to inform better athlete nutrition decisions.
These studies clearly show that diet and supplementation play an essential role in improving tennis athletes' performance. Nevertheless, it is crucial to consider individual factors and the specific needs of the athlete when designing an effective and safe nutritional strategy.
Nutrition's Impact on Stamina, Strength, and Recovery
Nutrition plays a crucial role in supporting stamina, strength, and recovery in tennis athletes. Carbohydrates, proteins, fats, vitamins, and minerals have a significant impact on these aspects.
1. The Role of Carbohydrates in Stamina
Carbohydrates are the body's primary energy source, especially in intense physical activities like tennis. Studies have shown that adequate carbohydrate intake can increase athletes' stamina and extend the time before feeling fatigued. A study by [23] stated that appropriate carbohydrate intake in quantity and timing can improve athletes' endurance and performance, including tennis athletes who require substantial energy during long matches.
2. Effect of Protein on Strength and Recovery
Protein is necessary for building and repairing muscles after training or competition. Adequate protein consumption can also increase muscle strength and speed up recovery. According to a study Ihsan & Nasrulloh, (2023), protein supplementation after training can increase muscle protein synthesis and accelerate the recovery of damaged muscles, contributing to long-term increases in muscle strength
3. The Importance of Fat in Long-term Stamina
Although often considered a reserve fuel, fat also has a vital role in supporting stamina, especially in training or competitions that last for extended periods. Fat can provide gradual and long-lasting energy. A study Cao et al., (2021) showed that a high-fat diet can increase fat oxidation and enable energy maintenance at low to moderate intensities, which is essential for tennis athletes in matches that last long periods.
4. Vitamins and Minerals for Optimal Recovery
Vitamins and minerals are essential to the body's recovery after training or matches. Some vitamins and minerals, such as vitamins C, E, and zinc, have anti-inflammatory and antioxidant properties that can help reduce inflammation and muscle tissue damage. Research [26] showed that adequate intake of vitamins C and E could reduce the extent of muscle damage and optimize the recovery process in athletes after strenuous exercise.
5. Water is an Essential Nutrient for Stamina and Recovery
Water is an often overlooked nutrient, being vital for athletes' stamina and recovery. Dehydration can lead to decreased performance, increased risk of injury, and slow recovery. A study [27] confirmed that dehydration of just 2% of body weight could decrease athlete performance, emphasizing the importance of maintaining adequate hydration during training and competition.
6. Electrolyte Supplements to Support Stamina and Recovery
Electrolytes such as sodium, potassium, and magnesium are essential for maintaining body fluid balance, muscle contraction, and nerve function. In situations where athletes lose a lot of fluid through sweat, electrolyte supplements can help maintain electrolyte balance and prevent fatigue and muscle cramps. According to a study [28], electrolyte supplements can reduce the risk of fatigue, decreased performance, and injury in athletes exposed to hot and humid environmental conditions.
A deep understanding of the relationship between nutrition and critical aspects such as stamina, strength, and recovery is essential for tennis athletes. By paying attention to proper nutrition, tennis athletes can improve their performance and prolong endurance and sustainability in intense matches.
Gaps in the Literature
The study of nutrition's effect on tennis athletes' performance has become an increasing focus in the scientific literature. However, although many studies have been conducted in this field, some gaps still need to be addressed. One of these is the lack of recent research that specifically examines the influence of nutrition on tennis athlete performance. While many studies have been conducted in this field, some gaps still need to be addressed. One of these is the lack of recent research that specifically examines the influence of nutrition on tennis athlete performance.
According to research [14], although there is increasing interest in the role of nutrition in sports, specific research on nutrition and tennis tends to be underrepresented in the current scientific literature. This could lead to a lack of in-depth understanding of the relationship between proper nutrition consumption and the improved performance of tennis athletes.
Furthermore, another gap in the literature is the need for more research considering specific aspects of nutrition and tennis, such as the role of nutrition in injury recovery in tennis athletes. A study [29] showed that proper nutrition can speed up the recovery process and reduce the risk of injury in tennis athletes. However, research explicitly examining nutritional strategies for injury recovery in tennis is limited.
Due to the need for more recent research on nutrition and tennis, it is essential to expand research that integrates more advanced methodologies, such as prospective cohort studies and sophisticated experimental designs. A study [30] emphasized the importance of sophisticated methodological approaches in sports nutrition research to better understand the relationship between nutrition and athletic performance.
In addressing this gap in the literature, researchers need to direct their efforts towards deepening the understanding of the specific types of nutrients that have the most effect on tennis athletes' performance, as well as how the timing of nutrient intake can affect performance during training and matches. A study [16] showed that nutrient intake before, during, and after practice or matches can significantly impact tennis athletes' performance.
The objective of this systematic review is to analyze and synthesize existing scientific evidence regarding the effect of nutrition on the performance of tennis athletes. This review aims to explore various nutritional strategies and dietary patterns commonly applied by tennis players, as well as examine the relationship between specific nutrients or supplementation and key performance indicators such as endurance, strength, agility, and recovery. By evaluating the effectiveness of these nutrition interventions, this study seeks to provide a clearer understanding of how nutrition contributes to athletic performance in tennis. Additionally, this review intends to identify gaps in the current literature and offer recommendations for future research to support the development of more effective and evidence-based nutritional strategies for tennis athletes.
MATERIALS AND METHODS OF RESEARCH
The research method used in this article was a systematic review that followed the PRISMA guidelines. This approach allowed for the structured collation and analysis of previous studies relevant to nutritional influences on tennis athlete performance. PRISMA provides a clear and systematic framework for identifying, assessing, and synthesizing evidence from the available literature in a transparent and detailed manner. The PRISMA approach requires a pre-defined research protocol, with inclusion (Table 1) and exclusion criteria, and a comprehensive search strategy. In addition, the methodological quality assessment of studies included in this review will be conducted systematically according to PRISMA guidelines. Using a PRISMA-guided systematic review approach, this study aims to provide a comprehensive and reliable synthesis of the relationship between nutrition and tennis athletes' performance based on the literature evidence.
Criteria Description Inclusion Study Type: Research articles (observational studies, intervention studies, meta-analyses, systematic reviews). Research Subjects: Professional or amateur tennis athletes of varying ability levels. Type of Intervention: Studies that evaluate the effects of nutrition (e.g., diet, supplements) on the performance of tennis athletes. Language: Studies published in English or other languages, provided there is a translation available. Publication Time: Articles published within the timeframe (2013 to 2024). Exclusion Study Type: Non-research reviews (editorials, newspapers, and book reviews). Study Subjects: Studies conducted on subjects other than tennis athletes or subjects with certain medical conditions. Type of Intervention: Studies that do not focus on nutritional interventions or only evaluate other aspects of performance. Language: Articles written in a language other than English for which there is no translation. Time of Publication: Articles published within more than 11 yearsTable 1. Inclusion Criteria ↓
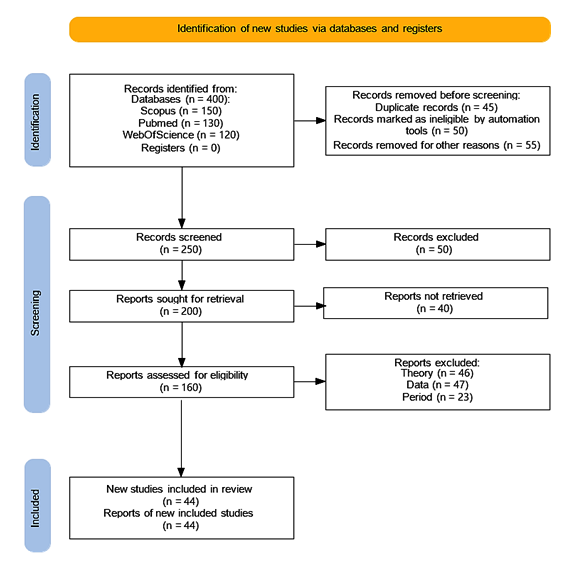
In the Selection Process stage, a literature search was conducted in reputable databases such as PubMed, Scopus, and Web of Science using related keywords such as "Tennis athlete nutrition," "Tennis supplementation and performance," and "athlete diet and physical fitness." The search was limited to articles published between 2013 to 2024 to ensure the inclusion of the most recent and relevant research. After the search, relevant articles were screened by title and abstract. Articles that fulfilled the inclusion criteria such as relevance to the research topic and appropriate research type were selected for full-text reading. Subsequently, articles that satisfy the requirements will be included in the analysis. During the selection process, article quality assessment criteria will also be applied to ensure methodological quality and relevance of findings to the research objectives. Using this approach, the most relevant and high-quality articles will be considered in the analysis, ensuring that the research has a solid and reliable foundation. The PRISMA flowchart illustrates the entire selection process, which increases transparency and makes it easier to understand the selection process (Fig.).
Figure. The PRISMA flowchart illustrates the entire selection process ↓
Data analysis in this study involved collecting and collating information from articles relevant to the topic. This process involved extracting data related to the nutrients studied, methods of measuring tennis athlete performance, and key findings from each article reviewed. The data were then analyzed to identify patterns or trends in the influence of nutrition on tennis athlete performance. The analysis approach may vary depending on the data collected, but generally includes grouping the data by relevant themes or variables and synthesizing the findings from the selected articles. Qualitative analysis methods may be used to understand the context and implications of the findings in depth.
In contrast, quantitative analyses, such as meta-analyses, may be used if sufficient data are available. Conclusions from these data analyses will help inform this systematic review's discussion and conclusions. PRISMA flowcharts will visualize the study selection and inclusion process, ensuring transparency and ease of understanding for the reader.
RESULTS AND DISCUSSION
In analyzing the findings regarding the influence of nutrition on the performance of tennis athletes, there are several essential aspects to consider (Table 2). First of all, carbohydrates, protein, and fat have a significant role in supporting the performance of tennis athletes. Carbohydrates are the primary source of energy for physical activity, which contributes to athletes' endurance and strength during matches. Research shows that adequate carbohydrate intake before and during matches can improve the performance of tennis athletes, especially in matches that require high intensity and last long [6]. On the other hand, protein is essential for maintaining and repairing muscles after training or matches. Adequate protein consumption can also help athletes build muscle mass and increase strength [36]. Fats, particularly healthy fats such as omega-3, have been shown to have anti-inflammatory effects that may help reduce the risk of injury and improve the cognitive function of tennis athletes [37].
Key Findings from Systematic Review Findings One of the supporting Journals of the Systematic Review Explanation Effects of Carbohydrate, Protein, and Fat [31, 32] Carbohydrate intake supports the stamina and energy that tennis athletes require during long, intensive matches. Protein has been shown to play an essential role in repairing and building muscle mass, which can help improve tennis athletes' physical strength and endurance. The right fats, especially polyunsaturated fats, can also support body function and nutrient absorption, essential for tennis athletes The Role of Vitamins and Minerals [1, 33, 34] Vitamins and minerals play a crucial role in supporting optimal body function, including strengthening the immune system, speeding up recovery, and maintaining electrolyte balance. Deficiencies in specific vitamins and minerals can negatively impact a tennis athlete's performance, that is why it is essential to ensure adequate intake of food or supplements Long-term and Short-term Impacts [14, 35] Proper nutritional intake can provide short-term benefits in improving performance immediately after consumption, as well as long-term benefits in sustaining and enhancing the performance of tennis athletes. Nutrients obtained from natural foods tend to provide better long-term benefits than nutritional supplements in maintaining athlete health and performanceTable 2. Findings in the Study ↓
In addition to macro-nutrients, vitamins, and minerals also have an essential role in improving the performance of tennis athletes. Vitamins such as vitamins C and E have antioxidant effects that can help in fighting oxidative damage that occurs during training or matches [21]. Minerals such as iron and calcium are also crucial for maintaining bone and muscle health and ensuring optimal muscle contraction during matches [38]. Proper nutritional intake can also help improve recovery and reduce the risk of injury in tennis athletes [39]. A consistent and balanced diet not only affects an athlete's performance immediately but can also have a long-term impact on an athlete's physical endurance from season to season [16].
Overall, the relationship between nutrition and tennis athlete performance is complex. Not only proper nutrition is necessary to improve current performance, but also to ensure the athlete's long-term health and reduce the risk of injury. Therefore, tennis athletes and coaching teams need to understand the importance of proper nutrition strategies and implement them in their training and competition. Thus, the effort required in planning and managing the diet of tennis athletes will not only help improve their current performance but will also provide long-term benefits to their health and career in the sport.
Importance of Nutrient Intake
Proper nutritional intake can contribute significantly to improving the stamina and strength of tennis athletes. Numerous studies have shown that sufficient carbohydrates can enhance physical endurance, which is a critical factor in long and intense tennis matches. For example, research [40] highlighted the importance of carbohydrates in improving long-term athletic performance by providing a sustainable source of energy for muscles during training and competition.
Proper nutrition also plays a vital role in supporting athletes' recovery process after training or competition. Protein, for example, is required to repair and rebuild muscles damaged during intense exercise or minor injuries during a match. According to research [41], adequate protein intake after training can increase muscle protein synthesis and accelerate muscle recovery associated with physical damage from exercise.
In addition to affecting physical aspects, nutritional intake can also have a positive impact on the mental and cognitive performance of tennis athletes. Specific vitamins and minerals, such as B-complex vitamins and magnesium, have been shown to play an essential role in neural function and mental concentration. A study [42] found that vitamin B complex supplements can improve cognitive performance and mood stability, which can benefit tennis athletes in maintaining focus and concentration during long, stressful matches.
While nutritional supplements are often an easy option, it's important to remember that natural sources of nutrients, such as whole foods, are also crucial for athletes' health and performance. A study by [43] highlighted that natural foods often provide nutrients in a more complete form and are easily absorbed by the body compared to supplements, which can have different side effects and tolerance in individuals.
By paying attention to proper nutrition intake, tennis athletes can maximize their physical and mental potential, improving endurance, strength, and focus, all of which are important in achieving peak performance in this demanding sport.
The results of this systematic review show that nutrition plays a crucial role in improving athlete performance. Interpretation of the findings suggests that various aspects of nutrition, such as carbohydrates, proteins, fats, vitamins, and minerals, have a significant impact on tennis athletes' stamina, strength, and recovery. For example, carbohydrates play an essential role in providing the energy required to endure intense training sessions and long matches. Proteins are needed to repair and build muscle after a workout or match. At the same time, fats provide lasting energy and aid in the absorption of specific vitamins that are essential for optimal body function.
The implications of these findings are clear. Tennis coaches, nutritionists, and athletes can use this information to design appropriate nutritional strategies to improve athlete performance. Practical recommendations include paying attention to the composition of meals before and after training sessions or matches, ensuring athletes have adequate intake of each type of nutrient required to maintain optimal health and performance. It is also essential to consider the individual needs of each athlete, as the body's response to nutrients can vary significantly between individuals.
However, while these findings provide valuable insights, some limitations need to be recognized. The systematic review method has the potential for bias in article selection and data interpretation. In addition, there are shortcomings in the literature that may affect the generalisability of the findings, such as the lack of studies examining the direct influence of nutrition on tennis athletes. This suggests the need for further research to understand more deeply the interaction between nutrition and performance in tennis athletes.
In the context of future research, it is essential to consider better research designs that allow the identification of causality between nutrient intake and the performance of tennis athletes. Longitudinal studies with larger samples may provide a more comprehensive insight into the impact of nutrition on tennis athletes' performance over time. In addition, there is a need for research that takes into account other factors that may influence the relationship between nutrition and performance, such as psychological and environmental factors.
In conclusion, while these findings provide strong evidence of the influence of nutrition on the performance of tennis athletes, further research is needed to understand in greater depth the complexity of this relationship. However, by paying attention to proper nutrition, tennis athletes can improve their performance and reach their maximum potential in their sport.
CONCLUSIONS
Acknowledgments.
The authors would like to thank all the team of authors included in this article who have helped in writing and analyzing this systematic review article very well.
Contributors:
Sayuty Yogi – conceptualization, validation, resources, funding acquisition, investigation, data curation, formal analysis;
Sabillah Muhamad Ichsan – software, writing – original draft, methodology, formal analysis, Investigation;
Hidayat Rezha Arzhan – data curation, visualization, supervision, project administration;
Sholichah Ima Fitri – writing – review & editing, software.
Funding. This research received no external funding.
Conflict of interests. The authors declare no conflict of interest.
REFERENCES
Key words: futsal, muscle fatigue, playing performance, physical condition
Ключові слова: футзал, м'язова втома, ігрова ефективність, фізичний стан
Abstract
This study investigates the impact of muscle fatigue on the physical condition and playing performance of futsal players, particularly focusing on decision-making, ball control, and technical skills under fatigue. Ten futsal players from Star Futsal Club (aged 17-25) participated in the study. Player performance was assessed using the Game Performance Evaluation Tool (GPET), which measured on-the-ball attacker and support actions, while physical condition was evaluated through shuttle run, 30-meter sprint, and vertical jump tests. The results showed a decline in performance after fatigue was induced. Specifically, the on-the-ball attacker score decreased from a pre-test mean of 81.00 to 71.75 post-test, and the support score dropped from 61.00 to 47.50. In terms of physical condition, the shuttle run time increased from a mean of 17.07 to 17.62 seconds, the 30-meter sprint time increased from 4.43 to 4.56 seconds, and vertical jump height decreased from 52.60 cm to 51.10 cm. Despite these observable declines, statistical analysis using paired samples t-tests revealed no significant differences: for player performance, t=5.353, df=1, p=0.118, and for physical condition, t=0.437, df=2, p=0.705. These findings suggest that muscle fatigue negatively impacts futsal players’ performance, particularly decision-making, speed, and technical execution, but the changes were not statistically significant, possibly due to the small sample size. The study highlights the importance of proper training load management and recovery strategies to optimize futsal performance. Further research with larger samples is needed to confirm these findings and better understand the effects of fatigue.
Реферат
Вплив м'язової втоми на ігрову продуктивність та фізичний стан футзалістів. Окта Йо., Субагіо І., Сабіллах М.І., Праното Н.В., Сапутра Д.Е.В., Фадзіллах Р.Н., Асмаваті П. Це дослідження вивчає вплив м'язової втоми на фізичний стан та ігрову ефективність гравців футзалу, зокрема на ухвалення рішень, контроль м’яча та технічні навички в умовах втоми. У дослідженні взяли участь десять футзалістів з клубу «Star Futsal» (вік 17-25 років). Оцінювання ефективності гравців здійснювалася за допомогою Інструменту оцінки ігрової ефективності (GPET), який вимірював дії гравців з м'ячем в атакуючих та підтримуючих ситуаціях, тоді як фізичний стан оцінювався за допомогою тестів на біг на шатл-руні, спринт на 30 метрів та вертикальний стрибок. Результати показали зниження ефективності після індукованої втоми. Зокрема, оцінка дій з м’ячем в атаці знизилася із середнього значення 81,00 до 71,75 після тесту, а оцінка підтримки – з 61,00 до 47,50. Щодо фізичного стану, час на шатл-руні збільшився з 17,07 до 17,62 секунди, час спринту на 30 метрів зріс з 4,43 до 4,56 секунди, а висота вертикального стрибка зменшилася з 52,60 см до 51,10 см. Незважаючи на ці спостережувані зниження, статистичний аналіз за допомогою парних t-тестів не виявив значущих відмінностей: для ефективності гравців t=5,353, df=1, p=0,118, і для фізичного стану t=0,437, df=2, p=0,705. Ці результати вказують на те, що м'язова втома негативно впливає на ефективність футзалістів, зокрема на ухвалення рішень, швидкість і технічне виконання, однак зміни не були статистично значущими, що, можливо, пояснюється малим розміром вибірки. Дослідження підкреслює важливість належного управління навантаженням і стратегій відновлення для оптимізації ефективності футзалу. Необхідні подальші дослідження з більшими вибірками для підтвердження цих висновків і кращого розуміння впливу втоми.
Today's athletes need external support to make progress in their sport. Sports science knowledge is one of the aspects that contribute to sports achievement. Combining several broad and interrelated scientific areas, sports science aims to enhance athlete performance and support coaches in their training [1, 2, 3]. Futsal is a ball game played by two teams, each consisting of five people, and played indoors [4, 5]. In general, the basic techniques in futsal are not much different from football. However, several basic techniques need to be done with special skills. The basic techniques in the game of futsal that must be mastered by every player include controlling the ball, passing, dribbling, and shooting [6, 7]. To be successful in futsal, players need to constantly be in top physical shape and work on improving their skills and accomplishments [8, 9]. In a variety of sports, the development of physical condition is fundamental to technical, tactical, and mental preparation [10, 11]. The setting up of physical conditions, strategies, tactics, and psychology is all related to one another. In sports activities, if your physical condition is not good, your technical, tactical, and mental abilities will result in less-than-optimal performance [12]. Good physical exercise is performed regularly, taking into account the body's capabilities and the appropriate amount of exercise [13, 14]. This requires physical, technical, and tactical training over a long period with an increasing workload, so it is hoped that players will develop good physical condition, mental strength, and technical skill [15].
Optimal physical condition is needed to combine the technical, tactical, and mental skills of players on the playing field. This is the basis that must be considered in efforts to achieve maximum athlete performance [16]. Every sporting activity contains elements of strength, duration, speed, and complex movements that require joint expansion [17]. This shows that to improve physical condition, the components of physical condition must be developed. Apart from that, the game of futsal requires players to play by moving the ball quickly, attacking, defending, and circulating the game without the ball or having the right time to make decisions [18]. Players must also master basic techniques such as dribbling, passing, control, chipping, and shooting. Basic techniques are very important to support playing performance on the field. There are various fundamental elements that contribute to developing physical fitness. Regarding the idea of muscular condition, the fundamental elements are endurance, strength, explosive power, speed, flexibility, agility, balance, and coordination [19, 20]. In futsal, the basic physical conditions that are dominant and must be possessed are speed, agility, and endurance because the characteristics of the game of futsal require these three components [21]. Therefore, players must be able to improve these abilities through physical training, as well as technical and tactical exercises, to achieve maximum performance. However, there is an effect of this training, namely that it will cause the players to experience fatigue. Training programs that are carried out progressively and continuously on players and exceed their limits will cause muscle fatigue. Over a long period, the muscles will eventually lose their ability to respond or contract due to fatigue. Apart from that, players can also experience pressure from outside, either environmentally or psychologically, which leads to stress.
Fatigue results in a lack of energy due to excessive physical activity [22]. In addition, physical activity can cause muscle pain and psychological discomfort. Fatigue is a major problem for athletes because it interferes with performance during competitions and can result in a decline in achievement [23]. When a player experiences fatigue, the player can still perform basic techniques such as dribbling, passing, control, and shooting [24]. However, players have difficulty making decisions and providing support, especially during movements without the ball that require speed. It can be concluded that there is an influence of fatigue on futsal playing performance.
Although many studies highlight the importance of recovery in supporting athletic performance, most existing research remains general and has not specifically examined the effectiveness of particular recovery methods in relation to specific sports, training intensity levels, and athletes' psychological conditions. Furthermore, there is a lack of studies that comprehensively integrate both physiological and psychological aspects in designing optimal recovery strategies. The purpose of this study is to investigate the impact of muscle fatigue on futsal players' performance and physical condition. Specifically, it aims to analyze how muscle fatigue affects the execution of fundamental skills such as dribbling, passing, ball control, and shooting, as well as decision-making during the game. Additionally, the study seeks to assess how muscle fatigue influences key physical components like speed, endurance, agility, and strength, and whether it impairs players' ability to maintain optimal physical condition throughout the match. Furthermore, the research will explore the relationship between muscle fatigue levels and overall physical performance decline, and how psychological factors, such as stress, interact with fatigue to affect technical execution and decision-making on the field. By addressing these factors, the study aims to provide a comprehensive understanding of how fatigue impacts futsal performance and inform more effective recovery strategies tailored to the needs of futsal athletes.
MATERIALS AND METHODS OF RESEARCH
This research uses a descriptive approach. Data is classified into two groups: quantitative data, which consists of numbers or symbols, and qualitative data, which is expressed in words. An instrument for assessing playing skills in soccer called the Game Performance Evaluation Tool (GPET) was employed in this study. The GPET evaluates coding decisions and execution in relation to the tactical challenges that players face during games [25]. Prior to participation, all subjects provided written informed consent after receiving a detailed explanation of the study’s objectives, procedures, and potential risks. The study was conducted in accordance with the ethical principles for human research. Ethical approval from the Ethics Committee of the Faculty of Sports Science, Universitas Negeri Surabaya is currently under review, and the protocol number will be provided upon completion of the approval process.
In this research, some aspects are assessed, namely (1) decisions made by players (Tactical Problem); (2) ball position when attacking (On-The Ball Attacker); (3) ball position when not attacking (Off-The Ball Attacker). Shuttle run is a form of agility training. Agility is defined as the body's ability to move and change direction in the shortest possible time without losing balance [26]. Agility is one of the components needed in the game of futsal. When dribbling the ball or trying to break through the opponent's defense, players must have good agility to perform optimally. The tools needed for a shuttle run are (1) Stopwatch; (2) Field; (3) Cones; and (4) Meter.
The study population consisted of ten futsal players selected using purposive sampling from the Star Futsal Club, aged 17-25 years. The selection criteria focused on core players who possessed greater experience and skill and were within the productive age range for optimal performance. The players were divided into two teams. Playing performance was assessed through futsal matches lasting 2×8 minutes, recorded for analysis. Physical condition tests included the shuttle run, 30-meter sprint, vertical jump, and a fatigue test using the Harvard step test for five minutes or until exhaustion, following a metronome pace of 120 beats per minute. Data analysis was conducted using SPSS version 26 (IBM Corp., Chicago, USA; license number WHIQVZYWLARL9JEYQEGDUBLH8Z3ZCJAL3FLXMS98V95TSDYI7FOEXUPRR).
Statistical tests included the Shapiro-Wilk test for normality, Levene’s test for homogeneity of variances, and paired samples t-tests to compare pre-test and post-test results for both player performance and physical condition. The statistical significance level was set at p<0.05. All results were presented as mean ± standard deviation (SD) and displayed in tables and figures for clarity.
RESULTS AND DISCUSSION
The research results were obtained based on observation of the pre-test and post-test results which were carried out by research subjects. The description of the pre-test and post-test data on the influence of muscle fatigue on physical condition and playing performance in futsal players from Star Futsal Club Klaten Regency is as follows:
1. Player performance data
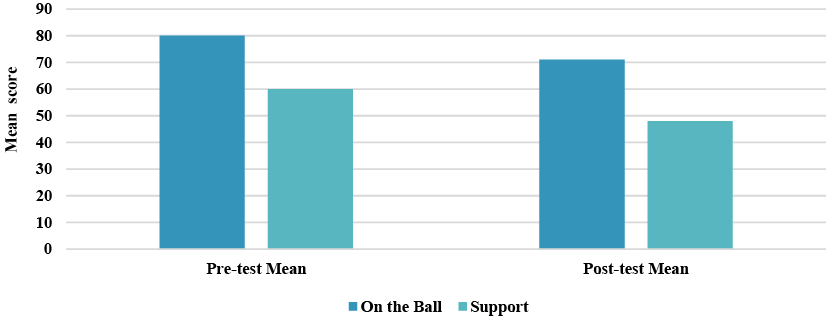
The mean pre-test value for on-the-ball attacker was 81.00, and the post-test value was 71.75. Meanwhile, the mean pre-test value for support was 61.00, and the post-test value was 47.50. The change in the mean values indicates a decrease in the subjects' playing performance. For more details, see Table 1 and Figure 1.
Statistics pre-test post-test on-the-ball attacker support on-the-ball attacker support Std. Dev 58.48 43.49 53.09 37.24 Min 20.00 16.00 15.00 10.00 Max 134.00 104.00 118.00 81.00 Mean 81.00 61.00 71.75 47.50 Note. Scores represent performance assessment points obtained from the observational instrument.Table 1. Pre-test and post-test results data of player performance ↓
Fig. 1. Differences between pre-test and post-test results data of player performance ↓
2. Physical condition data
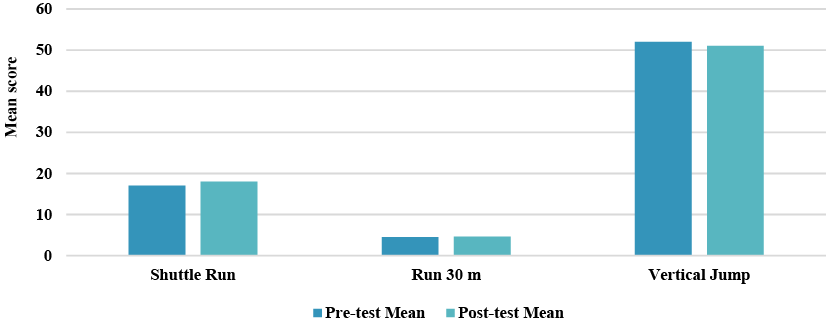
The results display the average, standard deviation, minimum, and maximum values in physical condition tests such as shuttle runs, 30-meter runs, and vertical jumps, based on study data. The data also include pre-test and post-test results. In the shuttle run test, the average pre-test score was 17.07 with a standard deviation of 0.53, and the post-test score was 17.62 with a standard deviation of 0.56. The mean pre-test result for the 30-meter run was 4.43 with a standard deviation of 0.24, and the mean post-test result was 4.56 with a standard deviation of 0.29. For the vertical jump, the pre-test mean was 52.60 with a standard deviation of 6.04, and the post-test mean was 51.10 with a standard deviation of 5.58. These findings suggest that fatigue leads to a decrease in physical condition, as shown by a reduced vertical jump. For more details, see Table 2 and Figure 2.
Statistics pre-test post-test shuttle run (seconds) run 30-meters (seconds) vertical jump centimeters (cm) shuttle run (seconds) run 30-meters (seconds) vertical jump centimeters (cm) Std. Dev 0.53 0.24 6.04 0.56 0.29 5.58 Min 16.24 4.17 44 16.97 4.34 43.00 Max 17.66 5.05 62 18.52 5.33 60.00 Mean 17.07 4.43 52.60 17.62 4.56 51.10 Note. Shuttle run and 30-meter run were measured in seconds (s), while vertical jump was measured in centimeters (cm).Table 2. Pre-test and post-test results data of physical condition ↓
Fig. 2. Differences between pre-test and post-test results data of physical condition ↓
To examine whether there is a statistically significant difference between the pre-test and post-test results, a paired samples t-test was conducted. This test is appropriate for assessing the effect of an intervention or treatment by comparing measurements taken from the same group before and after the intervention. The results of the analysis are presented in Table 3 below.
Measure t df p Pre-Test & Post-Test Player performance data 5.353 1 0.118 Pre-Test & Post-Test Physical condition data 0.437 2 0.705Table 3. Paired samples of T-test results ↓
The analysis revealed that the comparison of player performance data between pre-test and post-test resulted in a t-value of 5.353 with 1 degree of freedom (df) and a p-value of 0.118. For the physical condition data, the test produced a t-value of 0.437 with 2 degrees of freedom and a p-value of 0.705. Despite observable changes in both categories, neither result reached the conventional threshold for statistical significance (p<0.05). The p-values indicate that the differences in player performance and physical condition are not statistically significant. Therefore, based on the paired samples t-test, the observed differences between pre- and post-test scores may be due to chance rather than a meaningful effect of the intervention.
This research is important to conduct because futsal is a high-intensity sport that demands players to maintain optimal physical condition, possess solid technical skills, and make quick tactical decisions on the court. Fatigue, whether caused by intense training or frequent competition, can significantly impact performance in all these areas. In practice, fatigue is often overlooked or considered a normal part of training, but muscular fatigue that is not properly managed can lead to a noticeable decline in both physical and tactical performance. This study makes a valuable contribution by demonstrating how fatigue affects game performance both on-the-ball and off-the-ball actions as well as physical condition (speed, agility, and explosive power) in futsal players.
The findings of this research are supported by several previous studies. For example, researchers who developed the Game Performance Evaluation Tool (GPET) emphasized that decision-making and player positioning are key indicators of tactical performance in football and futsa [27]. This reinforces the validity of using GPET in this study to assess performance under fatigue. Additionally, [8] highlighted that speed, agility, and power are essential components in futsal performance, aligning with this study's focus. Furthermore, [18] stressed the importance of agility in handling the dynamics of futsal, supporting the need to maintain physical condition to optimize technical and tactical execution.
The implications of this study suggest that coaches and sports practitioners must account for fatigue when designing training programs and strategies during matches. Players experiencing fatigue exhibit reduced decision-making capabilities, positional awareness, and muscle power – all of which are crucial in futsal. Therefore, load management and appropriate recovery strategies must be prioritized. However, this study has several limitations. The small sample size of only 10 players from a single futsal club limits the generalizability of the findings. Additionally, psychological factors such as stress and motivation were not thoroughly examined.
This study highlights the impact of fatigue on futsal players' physical and tactical performance, but it has several limitations. The small sample size restricts the generalizability of the findings, and a larger sample would improve the external validity of the results. Additionally, the absence of a control group makes it difficult to determine if the observed performance changes were caused only by fatigue. Psychological factors such as stress and motivation were also not considered, yet they can significantly affect performance. Furthermore, potential learning effects between the pre-test and post-test could have influenced the results, as players may have improved simply due to familiarity with the testing procedure. For sports physiotherapists, it is crucial to monitor fatigue levels, as fatigue not only affects performance but also increases the risk of injury and decreases movement quality. Incorporating proper recovery strategies, such as active recovery exercises and load management practices, is essential. Future research should involve larger, more diverse samples and integrate psychological and physiological measurements to further understand the effects of fatigue and improve recovery and fatigue management strategies.
CONCLUSION
Contributors:
Ockta Yo. – validation, resources, writing – review & editing;
Subagio I. – methodology, software, validation, investigation, resources, data curation, supervision, writing – original draft, writing – review & editing;
Sabillah M.I. – conceptualization, validation, formal analysis, resources, writing – original draft, writing – review & editing, visualization, project administration;
Pranoto N.W. – validation, resources, writing – review & editing;
Saputra D.E.W. – validation, resources, writing – review & editing;
Fadzillah R.N. – validation, resources, writing – review & editing;
Asmawati P. – validation, resources, writing – review & editing.
Funding: This research received no external funding.
Conflict of interest: The authors declare no conflict of interest.
REFERENCES
Ключові слова: артрогенні контрактури, роботизована реабілітація, фізична терапія, Omego Plus, нижні кінцівки, ходьба, біль, функціонування, обмеження життєдіяльності
Key words: arthrogenic contractures, robotic rehabilitation, physical therapy, Omego Plus, lower extremities, walking, pain, limitations of activities of daily living
Реферат
В умовах воєнних дій в Україні значно зросла кількість пацієнтів із травмами кінцівок. Понад 60% втрат особового складу пов'язані з ускладненнями травм опорно-рухового апарату, зокрема артрогенними контрактурами. Резистентність таких станів до стандартної терапії зумовлює необхідність пошуку новітніх технологічних рішень, зокрема роботизованих систем з біологічним зворотним зв’язком “Omego Plus”. Мета: підвищення ефективності реабілітації пацієнтів з артрогенними контрактурами суглобів нижніх кінцівок шляхом клініко-функціонального обґрунтування та інтеграції в реабілітаційний процес роботизованої системи «Omego Plus». У рандомізоване дослідження було включено 60 пацієнтів (20-53 роки). Основна група (n=30) отримувала стандартну фізичну терапію (NICE-2022) та доповнену заняттями на системі «Omego Plus» (60 хв, 5 разів на тиждень, ). Контрольна група (n=30) займалася за стандартним протоколом. Оцінювання проводили поетапно (на початку дослідження, через 6 тижнів та через 3 місяці після виписки) за допомогою гоніометрії, (ММТ), візуально-аналогової шкали болю (ВАШ) та 10-метрового тесту (10MWT). В основній групі зафіксовано статистично високозначущу перевагу у відновленні згинання колінного суглоба до рівня функціональної норми (120 градусів, p=0,0005) та достовірний приріст амплітуди дорсального згинання стопи (p=0,0008). Аналіз м’язової сили виявив достовірно вищі абсолютні показники в основній групі на візиті 3 для відвідних м’язів (p=0,02) та внутрішніх ротаторів стегна (p=0,04), що свідчить про ефективніше рекрутування рухових одиниць роботизованої системи зі зворотним біологічним зв’язком «Omego Plus». Динаміка швидкості ходьби за тестом 10MWT підтвердила накопичувальний ефект роботизованої системи «Omego Plus»: міжгрупова перевага сформувалася на фінальному етапі оцінювання. Анальгезуючий ефект був найбільш вираженим між 2 та 3-м візитами (p<0,05), що вказує на стійкість результату та зниження явищ центральної сенситизації. Впровадження «Omego Plus» у післягострому періоді в основній групі забезпечувало відновлення мобільності рухів суглобів, збільшення силових показників та зниження больового синдрому. Результати обґрунтовують доцільність інтеграції роботизованої системи «Omego Plus» для подолання прогалин у реабілітації пацієнтів з артрогенними контрактурами.
Abstract
The impact of the robotic rehabilitation system with biological feedback "Omego Plus" on the functioning of patients with arthrogenic contractures of the joints of the lower extremities. Riahuzova O.T., Nekhanevych O.B., Lohvynenko V.V. Under the ongoing military actions in Ukraine, the number of patients with limb injuries has increased significantly. Over 60% of personnel losses are associated with complications from musculoskeletal injuries, specifically arthrogenic contractures. The resistance of such conditions to standard therapy necessitates the search for innovative technological solutions, particularly robotic systems with biofeedback, such as the "Omego Plus" system. Purpose. To enhance the effectiveness of rehabilitation for patients with arthrogenic contractures of the lower limb joints through clinical and functional justification and the integration of the "Omego Plus" robotic system into the rehabilitation process. This randomized controlled trial included 60 patients (aged 20-53 years). The main group (n=30) received standard physical therapy (NICE-2022 protocol) supplemented with sessions on the "Omego Plus" system (60 min, 5 times per week for 6 weeks). The control group (n=30) followed the standard protocol only. The assessment was carried out in stages (at the beginning of the study, after 6 weeks, and 3 months after discharge). Effectiveness was evaluated using goniometry, Manual Muscle Testing (MMT), the Visual Analog Scale (VAS) for pain, and the 10-Meter Walk Test (10MWT). A statistically significant advantage was observed in the main group regarding the recovery of knee flexion to the functional norm (120 degree, p=0.0005) and a significant increase in the amplitude of ankle dorsiflexion (p=0.0008). Analysis of muscle strength revealed significantly higher absolute values in the main group at Visit 3 for the hip abductors (p=0.02) and internal rotators (p=0.04), indicating more effective motor unit recruitment by the "Omego Plus" robotic system with biofeedback. Gait speed dynamics according to the 10MWT confirmed a cumulative effect of the "Omego Plus" system: the intergroup advantage was established during the final assessment stage. The analgesic effect was most pronounced between the second and third visits (p<0.05), indicating the stability of the result and a reduction in central sensitization phenomena. The implementation of "Omego Plus" during the post-acute period ensures rapid recovery of mobility, a significant increase in muscle strength indicators, and sustained reduction of the pain syndrome. The results justify the integration of the "Omego Plus" robotic system to address existing "gaps" in the rehabilitation of patients with arthrogenic contractures.
Захворювання та травмування опорно-рухового апарату розглядаються як одна з провідних причин формування хронічного больового синдрому, функціональної недостатності та стійкої дезінтеграції життєдіяльності пацієнтів у глобальному вимірі. Поєднання тривалої іммобілізації з комплексними ушкодженнями кісткових структур, нервових волокон та м’яких тканин формує чисельну когорту осіб з високим ризиком розвитку тяжких артрогенних контрактур, що зумовлює необхідність оптимізації та вдосконалення стратегій реабілітаційного втручання [3, 4, 5, 19].
Артрогенна контрактура – це стабільне обмеження активного та пасивного обсягу рухів, зумовлене патологічними змінами безпосередньо в його порожнині або навколишніх тканинах. В основі розвитку цього стану лежить поєднання хронічного запального процесу, деструкції хряща та фіброзного переродження періартикулярних структур, що сукупно формує стійку втрату мобільності суглобів. Клінічні наслідки контрактур охоплюють хронічний больовий синдром, порушення біомеханіки ходьби, підвищений ризик падінь. Тривалий функціональний дефіцит також корелює з розвитком психосоціальних порушень, зокрема депресивних симптомів, що знижує якість життя пацієнтів та підвищує їхню залежність від сторонньої допомоги [2, 3, 17, 21]
Проблема відновлення обсягу рухів у суглобах набула стратегічного значення для системи охорони здоров’я України внаслідок повномасштабної військової агресії. Це зумовлено безпрецедентним зростанням кількості пацієнтів з бойовою політравмою, зокрема поєднаними вогнепальними та мінно-вибуховими ураженнями опорно-рухового апарату. Згідно з актуальними даними, травми кінцівок є найбільш поширеними у структурі бойових ушкоджень, досягаючи 60,1% від загальної кількості санітарних втрат. Особливий механізм мінно-вибухової травми, на частку якої припадає до 95% поранень з лютого 2022 року, детермінує не лише гострий функціональний дефіцит, а й високу ймовірність формування стійких артрогенних контрактур у віддаленому періоді. Такий масштаб інвалідизуючих наслідків прогнозує системну кризу у сфері громадського здоров’я та вимагає негайної оптимізації реабілітаційних стратегій [9, 12, 19, 20]
Аналіз провідних профільних платформ та доказових баз даних з фізичної терапії (PEDro, Cochrane Library, Pubmed) свідчить про відсутність вузькоспеціалізованих клінічних настанов, присвячених безпосередньо менеджменту артрогенних контрактур. Наявна інформація здебільшого обмежена загальними принципами профілактики обмежень рухливості суглобів та рекомендаціями щодо ведення пацієнтів з м’язово-сухожилковими укороченнями. та методів втручання базується на дослідженнях на моделях тварин, результати яких потребують обережної інтерпретації та не можуть бути повноцінно екстрапольовані на складну клінічну картину [6, 15, 26].
Відсутність диференційованих протоколів фізичної терапії, які б ураховували специфіку стабільних артрогенних змін – таких як дегенерація хряща та фіброзна трансформація капсульно-зв’язкового апарату – створює суттєву наукову прогалину.
Для ефективності подолання цих викликів доцільно впроваджувати роботизовані системи. Вони дають змогу виконувати велику кількість повторень, що критично важливо для відновлення нормальної, фізіологічної роботи суглобів та м'язів. Застосування системи «Omego Plus» із функцією біологічного зворотного зв’язку дозволяє реалізувати диференційоване дозування механічного навантаження, що є важливим для ремоделювання тканин при артрогенній тугорухливості. Це не лише інтенсифікує терапевтичний процес, а й оптимізує роботу фахівця з фізичної терапії, нівелюючи надмірне фізичне навантаження [1, 2, 13, 14, 22, 23]
У нашому попередньому дослідженні було обґрунтовано та підтверджено ефективність застосування роботизованої системи «Omego Plus» з біологічним зворотним зв'язком у реабілітації пацієнтів з міогенними контрактурами нижніх кінцівок. Отримані результати засвідчили, що впровадження цієї технології дозволяє досягти зростання м'язової сили, збільшення обсягу рухів та збільшення швидкості ходьби на тлі вираженого зниження інтенсивності больового синдрому [14].
Однак у клінічній практиці важливою є диференціація обмежень рухливості за їхнім генезом. На відміну від міогенних контрактур, що мають високий реабілітаційний потенціал, артрогенні контрактури характеризуються значно вищою складністю відновлення через глибоку структурну перебудову суглобових елементів [3, 14]. Зважаючи на ці принципові патогенетичні відмінності, дані щодо ефективності роботизованої терапії при м'язових скороченнях не можуть бути автоматично екстрапольовані на випадки стабільних суглобових обмежень. Це зумовлює актуальність нашого поточного дослідження, спрямованого на верифікацію результативності системи «Omego Plus» у пацієнтів з артрогенними контрактурами нижніх кінцівок.
Метою дослідження є підвищення ефективності реабілітації пацієнтів з артрогенними контрактурами суглобів нижніх кінцівок шляхом клініко-функціонального обґрунтування та інтеграції в реабілітаційний процес роботизованої системи «Omego Plus».
МАТЕРІАЛИ ТА МЕТОДИ ДОСЛІДЖЕНЬ
Дослідження було проведене відповідно до вимог Гельсінської декларації Всесвітньої медичної асоціації «Етичні принципи медичних досліджень за участю людини в якості об’єкта дослідження». Усі пацієнти, які взяли участь у дослідженні, надали інформовану письмову згоду. Дослідження виконувалось у рамках науково-дослідної роботи кафедри фізичної реабілітації, спортивної медицини та валеології Дніпровського державного медичного університету «Медичне, фізіотерапевтичне та ерготерапевтичне забезпечення спортивних, оздоровчих та реабілітаційних тренувань» (№ 0121U114435, термін виконання 2022-2026 рр.) і було схвалено комісією з питань біомедичної етики Дніпровського державного медичного університету (протокол № 12 від 25.10.2023).
Дизайн дослідження: рандомізоване контрольоване дослідження з паралельними групами. Протягом 2024-2025 рр. у дослідження були включені 66 пацієнтів з артрогеними контрактурами суглобів нижніх кінцівок, із середнім віком 39,5 років, що отримували реабілітацію на базі відділення фізичної та реабілітаційної медицини КНП «Міська клінічна лікарня №4» Дніпровської міської ради» за програмою післягострого реабілітації. Критеріями включення були: діагноз посттравматичної контрактури одного або декількох суглобів нижньої кінцівки (кульшового, колінного, гомілковостопного) з обмеженням рухливості артрогенного походження з використанням оцінки патологічного кінцевого відчуття «жорстке», «пружинний блок», «капсулярний тип», що становить від 5% до 15% від норми, виміряний за допомогою гоніометрії [7, 10], старше 18 років, можливість самостійного пересування (з/без допоміжних засобів), загоєння післяопераційних ран (у разі оперативного втручання), надання письмової інформованої згоди на участь у дослідженні. Критерії виключення: використання апарата ої фіксації, ознаки декомпенсації серцево-судинних та інших захворювань, захворювання суглобів нижніх кінцівок в анамнезі, що призвели до стійкого обмеження рухливості, вроджені або набуті деформації суглобів нижніх кінцівок, недостатній рівень когнітивних функцій, що обмежує здатність розуміти інструкції фізичного терапевта (менше 24 балів за Монреальським когнітивним тестом (МоСА), за візуально-аналоговою шкалою (ВАШ), відмова в наданні інформованої письмової згоди на участь у дослідженні, наявність клінічних ознак ураження верхнього або нижнього рухового нейрона, наявність кінцевого відчуття «кістка до кістки» суглоба [2, 11]. За результатами застосування критеріїв виключення з дослідження вибули 6 пацієнтів, зокрема 1 особа мала апарат ьої фіксації, 3 пацієнти – запалення та активну фазу , 1 пацієнт – рівень МоСА 19 балів, 1 – відмовився надати згоду на участь у дослідженні.
Після застосування критеріїв включення-виключення в подальшому дослідженні продовжили участь 60 пацієнтів, яких розподіляли відповідно до рандомізаційної таблиці, що була заздалегідь сформована в сервісі Google Sheets (Google-таблиці), до двох груп (основну і контрольну) по 30 осіб в кожній. Сформовані групи не відрізнялись за віком, за статтю, (табл. 1). У дослідженні брали участь пацієнти у віці від 20 до 53 років, середній вік становив 39,5 (7,3) років, 26,7% з яких склали жінки, 73,3% – чоловіки, у контрольній – 93,3% чоловіки, жінки – 6,7% (р<0,05).
Показник Групи порівняння основна (n=30) контрольна (n=30) р Вік, роки 38,6 (7,8) 40,3 (6,8) 0,37 Стать Ч 22 (90,0 %) 28(95, 0%) 0,04 Ж 8 (10,0 %) 2 (5,0 %) Примітки: Ч – чоловіки; Ж – жінки; р – рівень статистичної значущості.Таблиця 1. Аналіз однорідності груп на початку дослідження за демографічними показниками(M(SD), n (%) ↓
Контрольна група отримувала стандартну фізичну терапію тривалістю 60 хвилин за заняття. Програма фізичної терапії для пацієнтів контрольної групи була розроблена на основі рекомендацій клінічної настанови NICE-2022 з реабілітації травматичних ушкоджень: тренування ходьби, вправи на розтягання, рівновагу, силу. Заняття проводились 5 разів на тиждень (4 тижні) під час стаціонарного етапу та 5 разів на тиждень (2 тижні) на амбулаторному етапі відповідно до пакетів медичних гарантій. У віддаленому періоді пацієнти виконували самостійну програму, спрямовану на збільшення гнучкості, сили, рівноваги та швидкості ходьби [NICE – 2022].
Крім стандартної програми на основі рекомендацій клінічної настанови NICE-2022 з реабілітації травматичних ушкоджень, пацієнтам основної групи призначали заняття з використанням роботизованої системи реабілітації зі зворотним біологічним зв’язком «Omego Plus». Програма реабілітації складалася з 60-хвилинних занять, спрямованих на розвиток витривалості та контроль рухів. Пацієнти виконували вправи з опорою на педалі роботизованого пристрою, де поступово зростав опір та збільшувався обсяг рухів у кульшовому, колінному суглобах. Розроблена програма фізичної терапії базувалася на застосуванні функціонально спрямованих тренувань тривалістю 60 хвилин, пріоритетними завданнями яких були розвиток загальної витривалості та вдосконалення нейром’язового контролю рухів. Центральною ланкою були втручання на роботизованому пристрої з біологічним зворотним зв'язком з використанням педальних модулів, що передбачало поступове кінематичне розширення (збільшення амплітуди рухів у кульшовому та колінному суглобах відповідно до функціональних можливостей пацієнта) та впровадження прогресуючого опору для інтенсифікації м’язової відповіді.
Для зміцнення м’язів-стабілізаторів застосовували режим, що поєднував ізотонічні рухи з короткочасною ізометричною експозицією (статичною фіксацією) у точках максимальної м'язової напруги. Окремий блок вправ був присвячений ізольованій зміні функцій гомілковостопного суглоба за допомогою спеціалізованих педалей із фіксацією стопи, який реалізовував рух виключно в площині плантарного згинання. Ця біомеханічна модель дозволяла акцентувати увагу на керованому ексцентричному навантаженні м’язів дорсального згинання, що є критично важливим фактором для відновлення фізіологічних фаз опору та переносу стопи під час ходьби.
Дозування фізичного навантаження здійснювалося за індивідуалізованим принципом на основі моніторингу об’єктивного статусу пацієнта шляхом гоніометрії цільових суглобів для визначення доступного безболісного діапазону рухів. Контроль реалізовувався за допомогою болю (ВАШ), допустимим порогом вважалася інтенсивність больового синдрому не більше 6 балів, при перевищенні якого рівень навантаження негайно коригувався. Додатково враховувалася суб’єктивна оцінка самопочуття пацієнта та наявність ознак загальної втоми під час заняття.
Оцінювання стану пацієнтів проводилось тричі: при надходженні (візит 1), у кінці 6 тижня (візит 2) та через 3 місяці після виписки (візит 3). За результатами кожного візиту програма фізичної терапії коригувалася, зокрема змінювалося дозування, тип та тривалість вправ. Для контролю виконання самостійних вправ пацієнти використовували електронний щоденник у Google-таблицях [16]. Його метою було відстеження прогресу в збільшенні обсягу рухів, сили та збільшення показників швидкості ходьби. Щоденник мав чітку структуру, включаючи розділи для фіксації даних гнучкості (назва вправи, кількість повторень, тривалість), сили (вага/повторення, підходи), рівноваги (час утримання, підходи) та тренування ходьби (тип, тривалість). Додатково пацієнти зазначали дату, суб'єктивну оцінку болю, загальне самопочуття та інші коментарі щодо прогресу. Комплексне обстеження пацієнтів базувалося на застосуванні інструментів та шкал, що дозволило забезпечити методологічне порівняння результатів з актуальними міжнародними даними [8, 24, 25]. Протокол оцінювання охоплював аналіз когнітивного статусу за допомогою Монреальської шкали (MoCA) [8, 18] верифікацію м’язової сили шляхом мануального м’язового тестування (MMT) та вимірювання обсягу рухів методом гоніометрії. Суб’єктивну інтенсивність больового синдрому фіксували за ВАШ, тоді як показники функціональної мобільності визначали за допомогою 10-метрового тесту (10MWT). Статистичний аналіз результатів дослідження проводили з використанням програми STATISTICA 6.1 (Statsoft Inc., США, ліцензійний № AGAR909E415822FA). Гіпотезу щодо нормальності розподілу показників оцінювали за критерієм Шапіро-Вілка. Нормально розподілені кількісні дані представлені у форматі М(SD), де М – середня арифметична величина, SD – середньоквадратичне відхилення, а ненормально розподілені – Mе (Q25;Q75), де Ме – медіана, Q25, Q75 – 25, 75 квартилі відповідно. Якісні дані представлені абсолютною кількістю спостережень (n) та відносною величиною (%). Оцінювання вірогідності відмінностей незалежних груп за кількісними показниками здійснювали за допомоги U-критерію Манна-Вітні, у пов’язаних групах – за критерієм Вілкоксона. Порівняльний аналіз за якісними показниками між групами проводився за критерієм хі-квадрат Пірсона. Відмінності вважали статистично достовірними за умови, що «р» менше 0,05 [12].
РЕЗУЛЬТАТИ ТА ЇХ ОБГОВОРЕННЯ
За результатами підсумкової гоніометрії суглобів нижніх кінцівок було встановлено, що пацієнти основної групи продемонстрували статистично високозначущу перевагу у відновленні активного згинання колінного суглоба (p=0,0005), досягнувши показників функціональної норми 120 градусів, тоді як у контрольній групі зберігалося клінічно виражене обмеження рухливості. При дослідженні гомілковостопного суглоба за показником активного дорсального згинання також було виявлено достовірну перевагу основної групи, у якій зафіксовано суттєвіший приріст амплітуди рухів порівняно з контрольною групою (p=0,0008). Оцінка функціонального стану кульшового суглоба засвідчила, що пацієнти обох груп досягли цільових показників активного згинання на момент завершення курсу реабілітації, проте в основній групі було зафіксовано вищі темпи відновлення амплітуди на проміжних етапах спостереження та вищу однорідність отриманих результатів у межах вибірки (мінімальна варіабельність значень), (табл. 2).
Хоча темпи зростання м’язової сили були схожими в обох групах, пацієнти основної групи досягли достовірно вищих абсолютних показників сили м’язів стегна, зокрема тих, що відповідають за відведення та внутрішню ротацію. Завдяки можливості системи «Omego Plus» точно дозувати навантаження було досягнуто значного зміцнення м'язів (табл. 3).
Аналіз результатів 10-метрового тесту (10MWT) виявив позитивну динаміку зростання швидкості ходьби в обох групах протягом усього курсу реабілітації. Проте порівняльний аналіз між групами показав, що статистично значуща перевага основної групи над контрольною сформувалася лише під час 3-го візиту. Хоча в основній групі спостерігалося достовірне покращення показників на кожному етапі (між 1, 2 та 3-м візитами), саме на завершальному етапі було зафіксовано міжгрупову різницю, що підтверджує кумулятивний ефект роботизованої терапії та її перевагу в довгостроковій перспективі відновлення швидкості та якості ходьби (рис. 1, 2).
Показник Групи порівняння основна (n=30) контрольна (n=30) р Згинання в кульшовому суглобі (Mе (Q25;Q75) 1 120,0 (100,0;120,0) 105,0 (100,0;120,0) 0,19 2 120,0 (120,0; 120,0) 112,5 (110,0;120,0) 0,06 3 120,0 (120,0:120,0) 120,0 (115,0;120,0) 0,01 ∆ 1-2 0,00 (0,00;10,0) 10,0 (0,00;10,0) 0,30 ∆ 1-3 0,00 (0,00;20,0) 0,00 (12,5;15,0) 0,80 Приведення в кульшовому суглобі 1 30,0 (25,0;30,0) 25,0 (20,0;30,0) 0,10 2 30,0 (30,0;30,0) 30,0 (30,0;30,0) 0,01 3 30,0 (30,0;30,0) 30,0 (30,0;30,0) 0,6 ∆ 1-2 0,00 (0,00;5,00) 5,00 (0,00;10,0) 0,46 ∆ 1-3 0,00 (0,00;5,00) 7,50 (0,00;10,0) 0,11 Згинання в колінному суглобі (Mе (Q25;Q75) 1 100 (80,0;110,0) 90,0 (90,0;100,0) 0,11 2 110,0 (100,0;120,0) 95,0 (85,0;105,0) 0,01 3 120,0 (110,0;120,0) 100,0 (90,0;110,0) 0,01 ∆ 1-2 10,0 (10,0;10,0) 5,00 (5,00;5,00) 0,002 ∆ 1-3 20,0 (10,0;30,0) 10,0 (10,0;10,0) 0,0005 Дорсальне згинання в ГС (Mе (Q25;Q75) 1 30,0(10,0;30,0) 5,00(5,00;10,0) 0,05 2 35,0 (20,0;35,0) 35,0 (35,0;40,0) 0,03 3 45,0 (35,0;45,0) 40,0 (40,0;45,0 0,7 ∆ 1-2 5,00 (5,00;10,0) 5,00 (5,00;10,0) 0,8 ∆ 1-3 15,0 (15,0;20,0) 10,0 (10,0;15,0) 0,0008 Примітки: 1,2,3 – візити; ∆ – різниця між візитами; р – рівень статистичної значущості.Таблиця 2. Аналіз динаміки обсягів рухів у суглобах нижніх кінцівок (M(SD) ↓
(Mе (Q25;Q75)
Показник сили Групи порівняння р основна (n=30) контрольна (n=30) М’язи, що відводять стегно, бали (Mе (Q25;Q75) 1 3,00 (3,00;4,00) 3,00 (2,00;3,00) 0,08 2 3,00 (3,00;4,00) 3,00(2,00;3,00) 0,08 3 4,00 (4,00;5,00) 4,00 (3,00;4,00) 0,02 ∆ 1-2 0,00 (0,00;0,00) 0,00 (0,00;0,00) 0,00 ∆ 1-3 1,00 (1,00;1,00) 1,00 (1,00;1,00) 0,16 М’язи, що виконують внутрішню ротацію, бали (Mе (Q25;Q75) 1 3,00 (3,00;4,00) 3,00 (2,00;3,00) 0,09 2 3,00 (3,00;4,00) 3,00 (2,00;3,00) 0,04 3 4,00 (4,00;5,00) 4,00 (3,00;4,00) 0,04 ∆ 1-2 0,00 (0,00;0,00) 0,00 (0,00;0,00) 0,32 ∆ 1-3 1,00 (1,00;1,00) 1,00 (1,00;1,00) 0,32 Примітки: 1, 2, 3 – візити; ∆ – різниця між візитами; р – рівень статистичної значущості.Таблиця 3. Аналіз динаміки сили м’язів нижніх кінцівок за мануальним м’язовим тестуванням ↓
Mean – середня арифметична величина, SE – стандартна помилка середньої величини, SD - середньоквадратичне відхиленняРис. 1. Різниця результатів 10-метрового тесту в процесі терапії, у комфортному темпі ↓
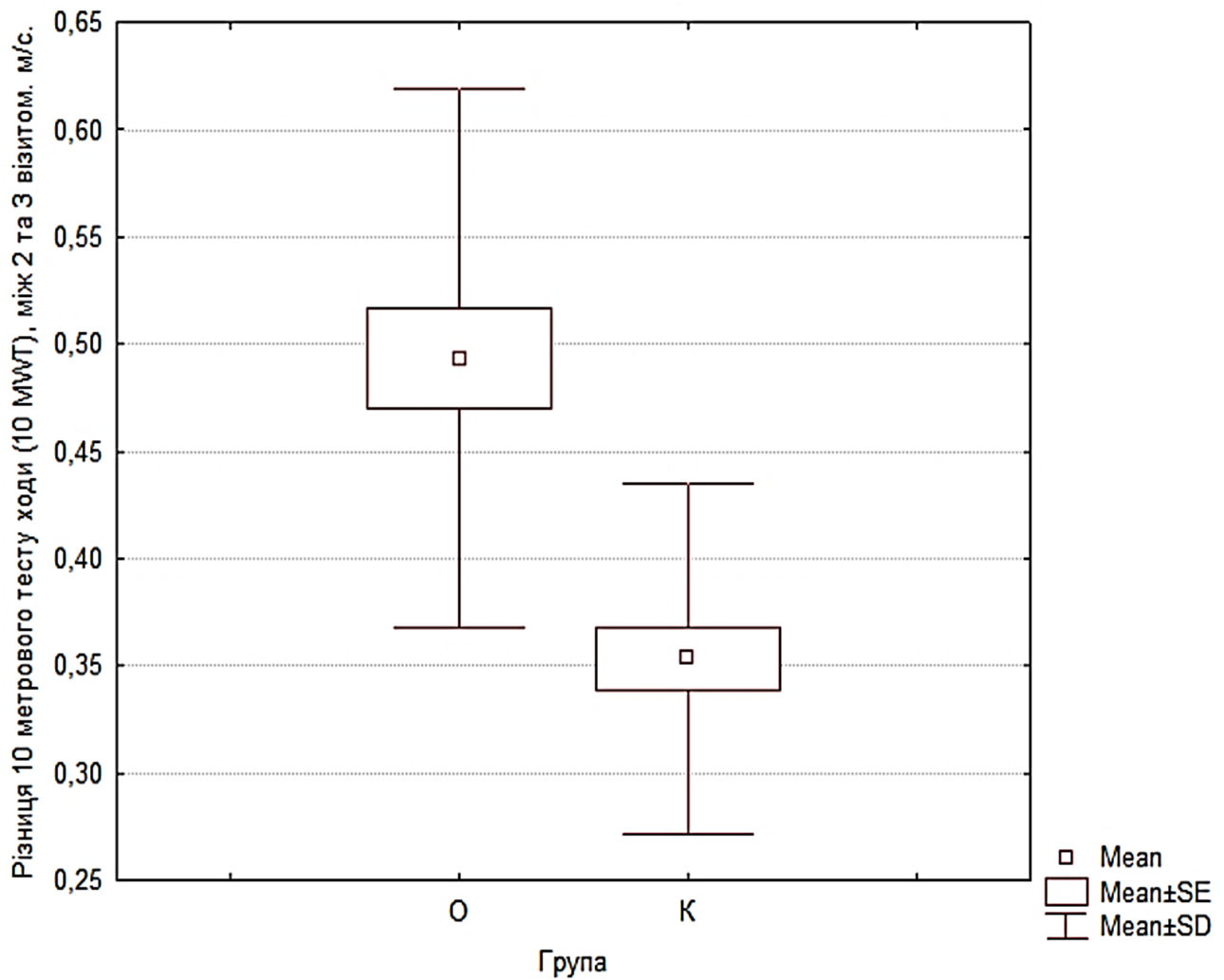
Mean – середня арифметична величина, SE – стандартна помилка середньої величини, SD - середньоквадратичне відхиленняРис. 2. Різниця результатів 10-метрового тесту в процесі терапії, швидка ↓
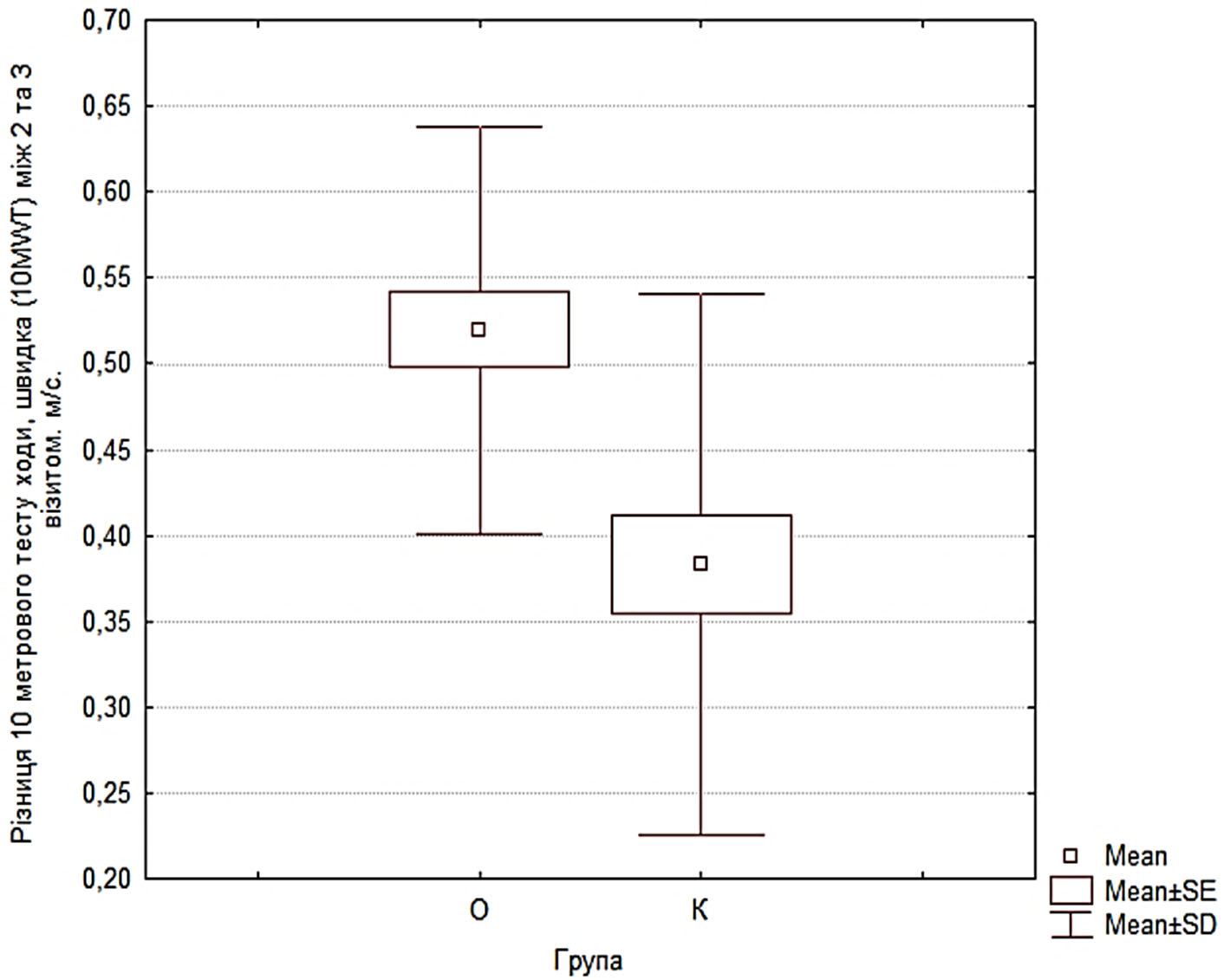
Упровадження роботизованої системи в протокол фізичної терапії підтвердило її високу ефективність у зниженні больового синдрому. В обох групах було зафіксовано зниження інтенсивності болю. Слід підкреслити наявність достовірної різниці показників саме між ІІ та ІІІ етапами оцінювання (p<0,05), що вказує на виражену позитивну динаміку у віддаленому періоді реабілітації. Така закономірність свідчить про анальгезуючий ефект застосованих методів та стійкість досягнутого терапевтичного результату на фінальних етапах відновлення (рис. 3).
ВАШ І, ІІ, ІІІ – рівень болю за ВАШ під час 1, 2, 3-го візитів відповідно, Mean – середня арифметична величина, SE – стандартна помилка середньої величини, SD – середньоквадратичне відхиленняРис. 3. Динаміка рівня болю за візуально-аналоговою шкалою у процесі терапії ↓
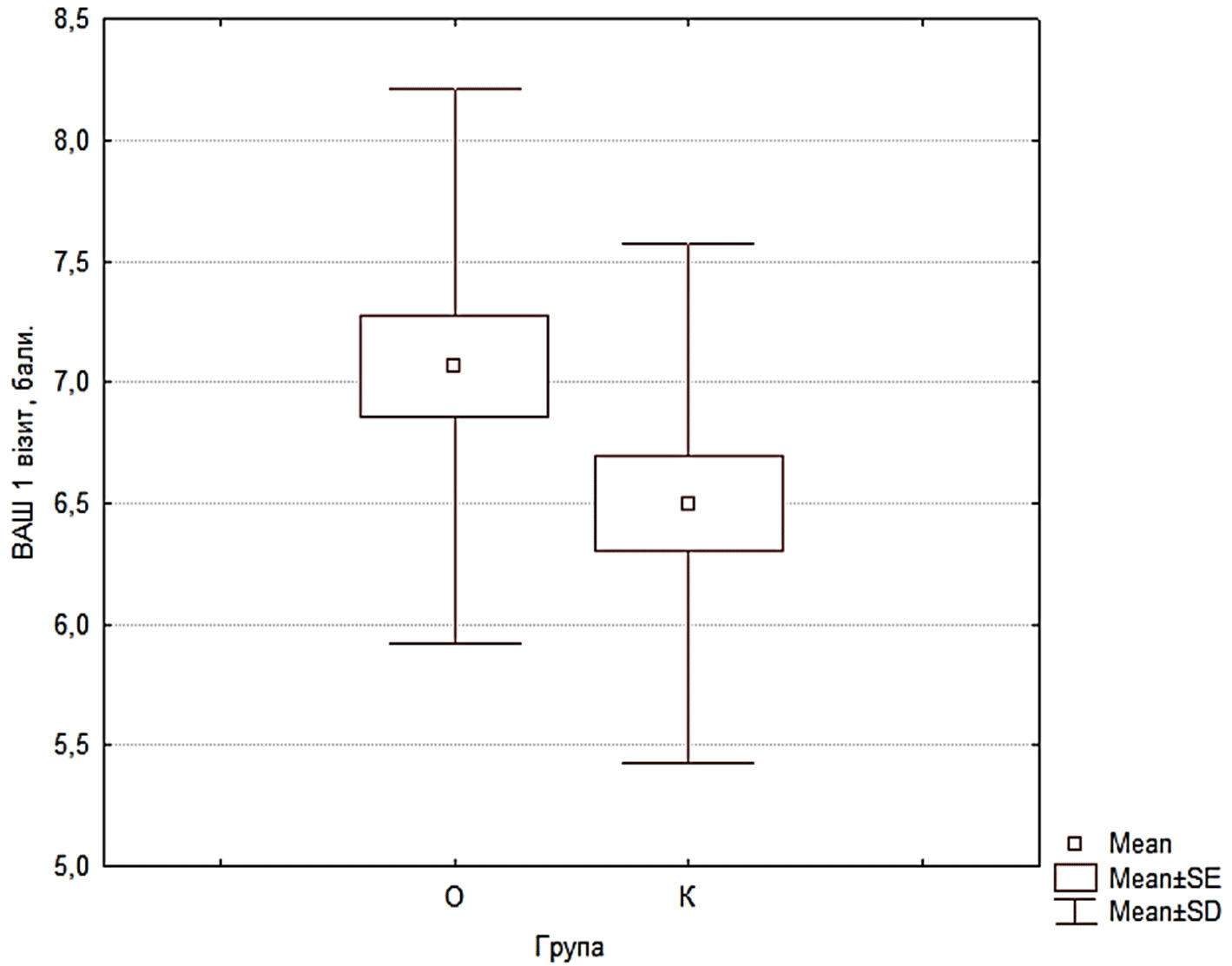
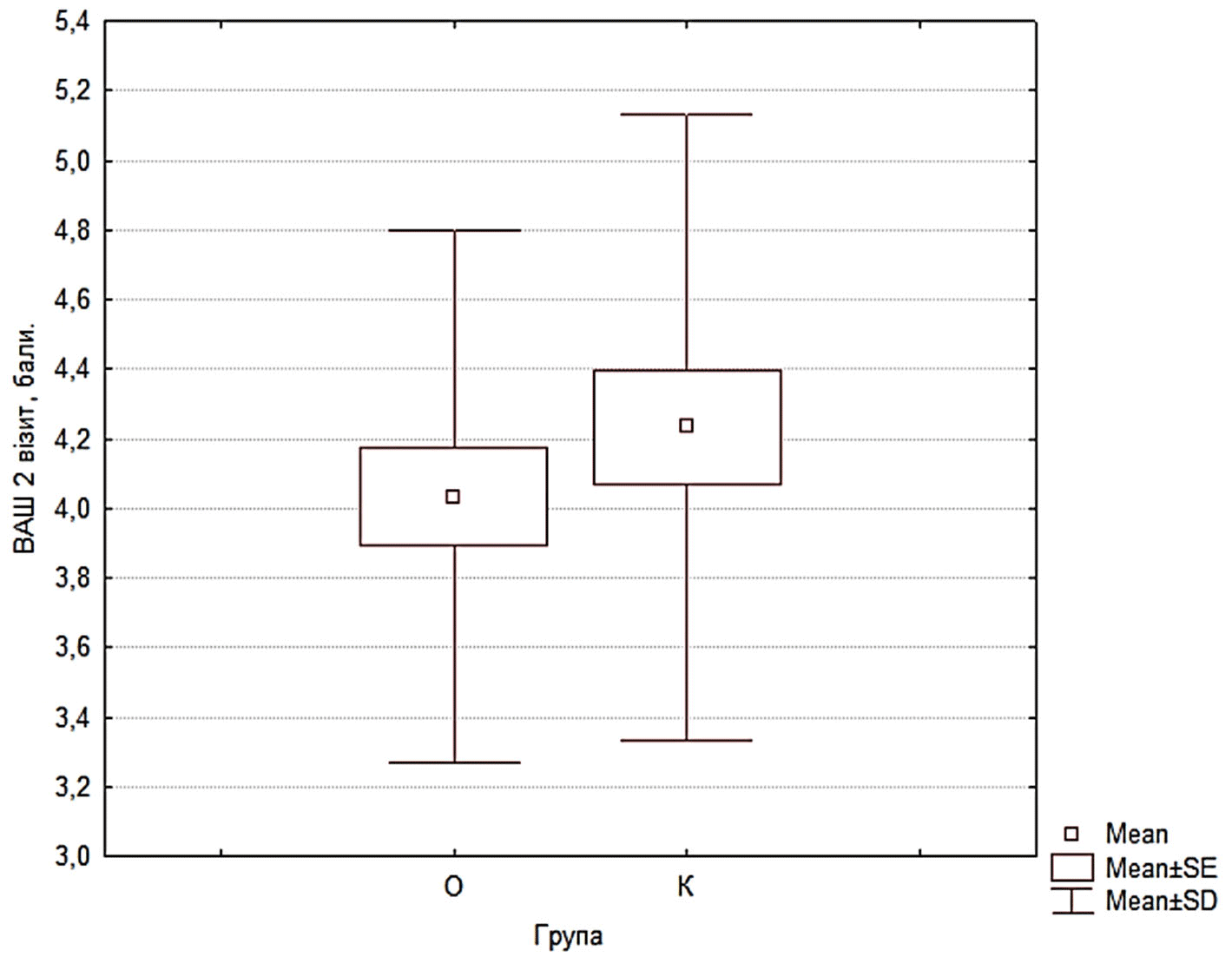
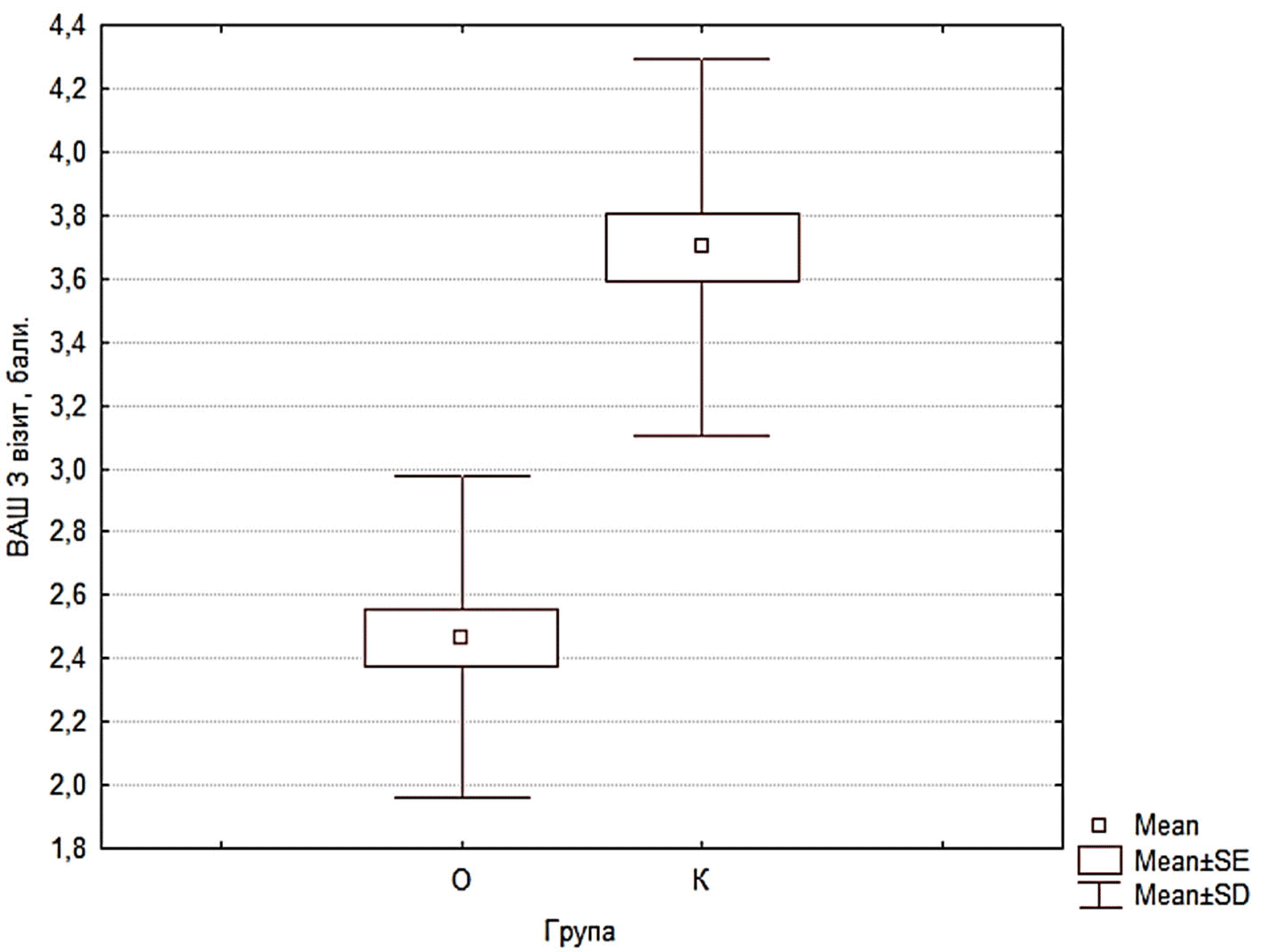
Отримані результати підтверджують гіпотезу про високу терапевтичну ефективність поєднання інтеграції роботизованої системи «Omego Plus» з акцентованим ексцентричним навантаженням. Досягнення пацієнтами основної групи функціональної норми згинання колінного суглоба 120 градусів зі статистично високозначущою перевагою над контрольною групою (p=0,0005) свідчить про те, що режим тренувань сприяє ефективнішому подоланню м'язової ригідності та іммобілізаційних контрактур. Ми припускаємо, що використання короткочасних ізометричних зупинок у точках максимальної напруги дозволяє оптимізувати нейром'язову відповідь та покращити пропріоцептивну аферентацію, чого важко досягти при стандартних пасивних або суто ізотонічних вправах. Особливої уваги заслуговує динаміка гомілковостопного суглоба: достовірний приріст амплітуди дорсального згинання (p=0,0008) в основній групі безпосередньо пов’язаний із застосуванням специфічного режиму педалювання. Використання педалей із фіксацією стопи забезпечило умови для ізольованого ексцентричного навантаження для дорсального згинання стопи, що є патогенетично обґрунтованим фактором відновлення еластичності м’язово-сухожилкового комплексу та підготовки пацієнта до фізіологічного перекату стопи під час ходьби. Хоча показники кульшового суглоба в обох групах досягли цільових орієнтирів, вищі темпи відновлення та низька варіабельність результатів в основній групі вказують на стабільність і прогнозованість роботизованого втручання. Це дозволяє стверджувати, що запропонований метод мінімізує вплив суб'єктивних факторів на процес реабілітації та забезпечує швидше досягнення клінічно значущого функціонального результату, що має важливе значення для скорочення термінів відновного лікування.
Аналіз динаміки м’язової сили дозволяє стверджувати, що застосування роботизованої системи «Omego Plus» забезпечує якісну перевагу у відновленні функціональної спроможності м’язів стегна. Попри те, що темпи зростання сили (∆ Ме) були порівняними в обох групах, статистично значуще вищі абсолютні показники в основній групі на момент завершення дослідження вказують на потужніший кумулятивний ефект розробленої програми. Досягнення вищих значень сили відвідних м’язів та внутрішніх ротаторів стегна (p=0,02 та p=0,04 відповідно) має ключове значення для стабілізації таза та забезпечення правильної біомеханіки ходьби, що часто є дефіцитарним показником при стандартній реабілітації.
Особливий інтерес викликає хронологія появи міжгрупових відмінностей. Більш раннє досягнення переваги в силі внутрішніх ротаторів (уже на візиті 2, p=0,04) може бути зумовлене специфікою роботи на педальних модулях, які вимагають постійної стабілізації стопи та гомілки, активуючи глибокі м’язи кульшового комплексу. Ми припускаємо, що збільшення силових показників у цьому випадку відбувається не лише за рахунок гіпертрофії м’язових волокон, а насамперед завдяки інтенсивному рекрутуванню рухових одиниць та покращенню нейром’язової координації. Використання роботизованої системи «Omego Plus» зі зворотним біологічним за стабільний опір та зворотний зв’язок, що дозволяє пацієнту точніше дозувати зусилля та активувати м’язові групи, які до цього не брали участь. Таким чином, запропонований підхід дозволяє швидше сформувати необхідний силовий потенціал для переходу до більш складних завдань для забезпечення потреби переміщень та ходьби, що скорочує загальний термін функціонального відновлення.
Аналіз динаміки швидкості ходьби за результатами 10-метрового тесту (10MWT) свідчить про стійку позитивну траєкторію відновлення локомоторної функції в обох досліджуваних групах. Проте виявлена закономірність, за якої статистично значуща міжгрупова перевага на користь основної групи сформувалася лише на етапі візиту 3, заслуговує на окрему увагу та патогенетичне обґрунтування.
Ми припускаємо, що такий відтермінований характер статистичної переваги є прямим доказом кумулятивного ефекту роботизованої терапії. На відміну від стандартних методів, роботизована система забезпечує високу інтенсивність та прецизійну повторюваність циклічних рухів, що є критичним для консолідації нових рухових патернів. Відсутність міжгрупової різниці на етапі візиту 2 при наявності достовірного внутрішньогрупового покращення вказує на те, що перші тижні реабілітації були періодом накопичення функціонального потенціалу (збільшення амплітуди рухів та сили м’язів).
Перевага, зафіксована на завершальному етапі (візит 3), вказує на успішну функціональну інтеграцію отриманих біомеханічних приростів у цілісний акт ходьби. Вища швидкість ходьби в пацієнтів основної групи на момент завершення курсу підтверджує, що застосований протокол дозволяє не лише покращити окремі параметри (силу чи об’єм рухів), а й трансформувати їх у якісну зміну спроможності функції ходьби. Таким чином, роботизована терапія демонструє вищу ефективність у довгостроковій перспективі, забезпечуючи кращу адаптацію пацієнта до щоденних функціональних навантажень.
Упровадження роботизованої системи «Omego Plus» зі зворотним біологічним зв’язком у протокол фізичної терапії засвідчило її суттєвий анальгезуючий потенціал. Позитивна динаміка зниження інтенсивності больового синдрому в обох досліджуваних групах підкреслює фундаментальну роль контрольованої рухової активності в процесах модуляції ноцицептивної відповіді. Проте виявлена статистично значуща різниця показників саме між ІІ та ІІІ етапами оцінювання (p<0,05) вказує на виражений накопичувальний характер терапевтичного впливу та його особливу ефективність у довготривалому періоді реабілітації. Ми припускаємо, що така закономірність зумовлена поступовою функціональною адаптацією нейром’язового апарату до навантажень та поступовим зниженням явищ центральної сенситизації на фоні відновлення фізіологічної біомеханіки рухів. Використання роботизованої системи дозволяє забезпечити прецизійне дозування амплітуди та опору, що мінімізує ризик механічного подразнення тканин і сприяє стійкому регресу болю. Стійкість досягнутого результату на завершальному етапі відновлення підтверджує, що запропонована методика сприяє формуванню стабільних компенсаторних механізмів, що має вирішальне значення для підвищення комплаєнсу пацієнтів та успішної реалізації складніших функціональних завдань.
Таким чином, клініко-функціональне обґрунтування інтеграції роботизованої системи «Omego Plus» у протокол реабілітації пацієнтів з артрогенними контрактурами дозволило сформулювати низку стратегічно важливих висновків, що доповнюють та розширюють сучасну доказову базу.
1. Терапевтична специфічність при артрогенних ураженнях
Це дослідження спрямоване на усунення суттєвої наукової прогалини в менеджменті контрактур суглобів. У той час, як більшість наявних клінічних настанов зосереджені на корекції міогенних скорочень [15], наша робота вперше демонструє високу ефективність роботизованої терапії при артрогенних змінах, які характеризуються резистентністю до стандартної фізичної терапії через глибоку структурну перебудову суглобових елементів. Верифікація результативності методу в цій складній когорті пацієнтів є логічним продовженням попередніх напрацювань [14] та вказує на ширший терапевтичний діапазон системи «Omego Plus» порівняно зі стандартними методами механотерапії.
2. Досягнення функціональних цільових результатів та нейром’язова оптимізація
На відміну від багатьох досліджень, що фіксують лише загальне покращення мобільності [1, 22, 23], отримані нами дані свідчать про досягнення клінічно значущої функціональної норми (згинання колінного суглоба 120 градусів, p=0,0005). Такі результати є прямим наслідком застосування розробленого динамічного режиму. Особливу наукову новизну становлять дані щодо прецизійного зміцнення м’язів-стабілізаторів: достовірно вищі абсолютні показники сили відвідних м’язів та внутрішніх ротаторів стегна (p=0,02 та p=0,04 відповідно) підтверджують гіпотезу про здатність роботизованої системи з біологічним зворотним зв’язком забезпечувати ефективніше рекрутування рухових одиниць глибоких м’язових груп.
3. Кумулятивна траєкторія відновлення та нейромодулюючий ефект
Аналіз результатів виявив специфічну часову закономірність відновлення локомоторної функції та модуляції болю. Формування статистично значущої міжгрупової переваги у швидкості ходьби (10MWT) виключно на завершальному етапі (візит 3) обґрунтовує кумулятивний характер роботизованого втручання, необхідний для стійкої нейромоторної адаптації та інтеграції біомеханічних приростів у цілісний патерн ходьби. Водночас пролонгований регрес больового синдрому, найбільш виражений на фінальних етапах втручання (p<0,05), вказує на нейромодулюючий вплив циклічного роботизованого навантаження. Це дозволяє стверджувати, що застосований протокол сприяє зниженню явищ центральної сенситизації та формуванню стабільних компенсаторних механізмів. Таким чином, інтеграція «Omego Plus» у післягострому періоді забезпечує не лише швидку корекцію окремих функцій, а й якісно вищий рівень нейром’язового контролю, результати якого залишаються стійкими в катамнестичному періоді спостереження.
ВИСНОВКИ
Внески авторів:
Рягузова О.Т. – ресурси, концептуалізація, методологія, проведення дослідження, курація даних, формальний аналіз та інтерпретація, написання – початковий проєкт, написання – рецензування та редагування;
Неханевич О.Б. – концептуалізація, написання – початковий проєкт, написання – рецензування та редагування, ведення, адміністрування проєкту;
Логвиненко В.В. – перевірка, написання – рецензування та редагування.
Фінансування. Дослідження не має зовнішніх джерел фінансування.
Конфлікт інтересів. Автори заявляють про відсутність конфлікту інтересів.
REFERENCES
Key words: creatine kinase, physical exercise, physical fitness, muscle damage
Ключові слова: креатинкіназа, фізичні вправи, фізична форма, пошкодження м’язів
Abstract
Creatine kinase (CK) is a key enzyme in cellular energy metabolism, playing a role in the regeneration of adenosine triphosphate through the phosphocreatine system, particularly in tissues with high energy demands such as skeletal muscle. Under normal conditions, CK is present within muscle cells, so its blood levels are relatively low. However, strenuous or unusual physical exercise especially with eccentric contractions can cause mechanical and metabolic stress that disrupts muscle fiber integrity and increases cell membrane permeability. Microdamage to the sarcolemma, accompanied by oxidative stress, inflammatory responses, and disruption of intracellular calcium homeostasis, are thought to cause the release of CK from muscle cells into the bloodstream. Although CK is widely used as a biomarker of exercise-induced muscle damage, its increased levels do not always correlate directly with the degree of muscle damage or functional impairment, so the exact mechanism of post-exercise CK release remains incompletely understood. The aim of this study was to determine the effect of physical exercise on increasing CK levels. We reviewed several literature databases, including Scopus, Pubmed, Web of Science, and Science Direct, for our systematic review investigation. The search was conducted for articles published between 2015-2025 that discussed physical exercise and CK. Using the Scopus, Web of Science, Pubmed, and Science Direct databases, 1,450 published publications were identified. For this systematic review, nine papers that met the inclusion criteria were selected and reviewed. This study evaluated the standard operating procedure using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Based on 9 reviewed papers it has been proven that physical exercise has been proven to increase CK levels significantly. Exercise-induced CK elevations serve as a valuable, albeit nonspecific, indicator of muscle damage. Understanding the variability in CK responses is critical to designing training and recovery programs for athletes in order to achieve optimal physical performance.
Реферат
Зміни креатинкінази, викликані фізичними вправами: систематичний огляд. Путро Б.Н., Вібава Дж.К., Аюбі Н. Креатинкіназа (КК) – ключовий фермент клітинного енергетичного метаболізму, що відіграє роль регенерації аденозинтрифосфату через фосфокреатинову систему, особливо в тканинах з високими енергетичними потребами, як-от скелетні м’язи. За нормальних умов КК присутній у м’язових клітинах, тому його рівень у крові відносно низький. Однак інтенсивні або незвичайні фізичні навантаження, особливо з ексцентричними скороченнями, можуть викликати механічний та метаболічний стрес, який порушує цілісність м’язових волокон та збільшує проникність клітинної мембрани. Вважається, що мікроушкодження сарколеми, що супроводжуються окиснювальним стресом, запальними реакціями та порушенням внутрішньоклітинного кальцієвого гомеостазу, призводять до вивільнення КК з м’язових клітин у кровотік. Хоча КК широко використовується як біомаркер пошкодження м’язів, викликаного фізичними вправами, її підвищений рівень не завжди прямо корелює зі ступенем пошкодження м’язів або функціональними порушеннями, тому точний механізм вивільнення КК після тренування залишається недостатньо вивченим. Метою цього дослідження було визначення впливу фізичних вправ підвищення рівня КК. Для проведення систематичного огляду ми проаналізували кілька баз даних наукової літератури, включаючи Scopus, PubMed, Web of Science та Science Direct. Пошук проводився за статтями, опублікованими в період з 2015 до 2025 року, у яких обговорювалися фізичні вправи та КК (креатинкінази). За допомогою баз даних Scopus, Web of Science, PubMed та Science Direct було виявлено 1450 опублікованих робіт. Для цього систематичного огляду було відібрано та проаналізовано дев'ять статей, що відповідають критеріям включення. У цьому дослідженні оцінювалася стандартна робоча процедура з використанням PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). З аналізу 9 статей було доведено, що фізичні вправи значно підвищують рівень КК. Підвищення рівня КК, викликане фізичними вправами, є цінним, хоч і неспецифічним індикатором ушкодження м’язів. Розуміння варіабельності реакції КК має вирішальне значення для розробки тренувальних і відновлювальних програм для спортсменів з досягнення оптимальної фізичної працездатності.
Physical exercise is known as a non-pharmacological therapy in an effort to improve the health and standard of living of humans. However, physical exercise, in addition to making you healthy, also triggers certain conditions that result in an imbalance in the body's homeostasis if not done properly and correctly according to WHO recommendations. A rise in ROS (reactive oxygen species) is another indicator that physical activity causes oxidative stress [1]. Exercise causes the body's oxygen consumption to rise by 20-100 times greater than usual, making it impossible for the oxygen supply to keep up [2]. It is well recognized that the body contains a number of ROS, such as hydrogen peroxide (H2O2), hydroxyl radicals (OH-), and superoxide anions (O2-). When physical exercise causes stress, these ROS are known to be essential for cellular physiological functions [3]. During exercise, skeletal muscles also help produce ROS, which is essential for gene expression, cellular signal transduction, strength enhancement, and muscle mass maintenance. However, excessive ROS levels will interfere with muscle contraction and performance continuity [2]. However, we are all aware that excessive ROS production during exercise can lead to oxidative stress, which exacerbates existing medical issues [3]. The body's overproduction of ROS can potentially damage cell biomacromolecules, leading to aging, muscle cell death, and damage to lipids, proteins, and nucleic acids physiological events that happen during physical activity [4]. Apart from that, ROS is a normal physiological reaction that happens during exercise to initiate additional signal transductions [5].
The main cause of exercise-induced muscle damage (EIMD) is unfamiliar physical activity, particularly if it includes a lot of eccentric contractions [6]. Along with a brief loss of muscle strength, this breakdown process usually causes delayed onset muscle soreness (DOMS), which usually starts a few hours after activity and peaks gradually over a few days [7]. In recent decades, numerous ideas have been proposed to explain the process of deterioration [8], however, the precise process remains unclear. After a great deal of fascial research in recent years, it has been shown that fascia is the main cause of pain during eccentric exercise [9]. Additionally, during DOMS episodes, deep fascial shear dysfunction has been noted, and this is correlated with later DOMS recovery [10]. Therefore, the function of fascial sliding may have a significant impact on DOMS; however, a thorough investigation of this link has not yet been conducted. Additionally, there are biomarkers, including creatine kinase (CK), that indicate muscle injury.
The enzyme creatine kinase (CK), sometimes referred to as creatine phosphokinase, is involved in the synthesis of energy. Tissues that consume a lot of energy, such as the brain and muscles, especially the heart, have higher quantities of this enzyme. Serum CK enzyme levels range from 20-35 to 200-400 U/L at baseline [11]. When exercise damages the skeletal muscle cell structure in the sarcolemma and Z-disc levels, creatine kinase will leak into the circulation [12]. The proportional amount of CK produced, the degree of CK enzyme activity released, and the rate of CK clearance from the blood will all be reflected in the measured serum CK [13]. Additionally, it has been proposed that muscle cells "voluntarily" release adenosine triphosphate (ATP)-consuming enzymes like CK in order to avoid cell death under crucial metabolic conditions [14]. Instead of linking CK to "muscle damage," some studies now associate it with "membrane damage" or "membrane permeability." One qualitative marker of muscle injury, especially in the context of endurance exercise, has been suggested to be elevated plasma CK activity [15]. Serious muscle problems are generally thought to be indicated by serum CK values greater than 5000 U/L [14]. CK has also been proposed as an indicator of recovery, but due to high variability in baseline levels or in response to exercise, there is no general consensus. The underlying mechanism by which exercise can raise CK levels as a sign of muscle injury and the consequences for day-to-day living are still unknown. To accurately explain how CK reacts during exercise, it is crucial to understand its phases and mechanisms. Therefore, the aim of this study was to examine in-depth how physical exercise affects CK levels and to examine the underlying mechanisms.
MATERIALS AND METHODS OF RESEARCH
This study was a systematic review, in which the researchers conducted extensive searches through journal databases such as PubMed, Science Direct, Web of Science, and Scopus. These databases are considered to be the world's largest for collecting high-impact papers with a strong scientific foundation, ensuring their legitimacy and validity are undeniable. Using this first-come, first-served search method, duplicate articles were removed. Using predetermined inclusion and exclusion criteria, the search results were then further refined.
The inclusion criteria for this study were developed reviewing publications since 2015 to 2025 that addressed physical activity and creatine kinase. Additionally, journals that did not adhere to scientific validity requirements or were not listed in reliable search indexes like Scopus, Web of Science, Pubmed, or Science Direct were not included in our research.
The full texts, abstracts, and titles of the papers were added to the Mendeley database after initial evaluation and confirmation. In the first phase, 1,450 publications were found using the databases Scopus, Science Direct, Pubmed, and Web of Science. After the title appropriateness screening, 734 acceptable papers were selected for the second screening stage (Fig.). Following a review of the title, abstract, and keywords, 166 papers were selected for the third round. Upon reviewing each publication, we determined that they matched the inclusion requirements, which include the following: the study must be original, the parameter must be a creatine kinase biomarker, the intervention must be physical activity of any kind, and the sample must be human. At this point, we organized the items based on their overall suitability. Nine papers that met the inclusion criteria were selected for analysis after a thorough review and observation process. The operational requirement for this study was to comply with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). In addition, all papers have met research ethics and are in accordance with the Helsinki Declaration.
Fig. PRISMA flowchart of the article selection process ↓
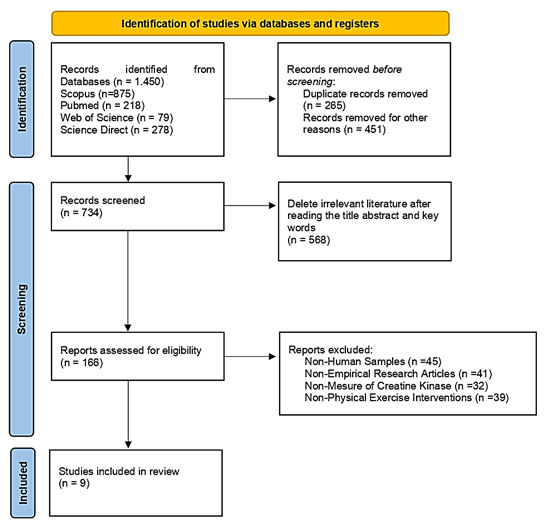
RESULTS AND DISCUSSION
Author Design Participants Participants Age Intervention Outcome (Chen et al., 2025) [6] Randomized controlled trials 24 males 18-25 years Exercise Program Eccentric exercise with The following is the Active range of motion is 30° Participants only do eccentric workouts while seated on the dynamometer Eccentric exercise has been shown Intervention of tissue flotation after eccentric exercise inhibits the increase in creatine kinase (Santos Cerqueira et al., 2021) [16] Randomized controlled trials Thirty healthy young men 18 to 35 years Exercise Program Participants performed A total of 10 sets The volunteer's knees were passively positioned at a 30° angle (0°=total extension) before each contraction. Subjects were instructed Participants were instructed Eccentric training has been shown to significantly increase creatine kinase levels after intervention (Allard et al., 2023) [17] Randomized controlled trials Hundred 62-66 years Exercise Program Participants of the Nijmegen March walk Each day, participants walked 30, 40 and 50 kilometers. For four consecutive days, the exercise intervention was conducted There was a significant increase in CK levels at its peak 2 days after exercise and on the third day CK levels tended to decrease. (Bray et al., 2025) [18] Randomized controlled trials Eleven senior club male fast bowlers 27.3±7.0 years Exercise Program The CA-AIS fast bowling skills test is finished by participants. To put it briefly, bowlers The other players finish a physical exercise that simulates fielding in the interim. There was a significant increase in CK levels immediately after the intervention (D’Alleva et al., 2025) [19] Randomized controlled trials Seventeen participants 40 years Exercise Program Twenty-four weeks Warming up is done before treatment. Following that, runners might choose to run a half, thirty, or full marathon. There was a significant increase in CK levels immediately after the marathon running intervention. (Biss et al., 2023) [20] Randomized controlled trials Twelve healthy participants 18-45 years Exercise Program Stand, squat, biceps curl, toe stand with whole body extension, and other exercises included in the book are examples of electromyostimulation exercises. Plank, deep squat, knee tuck walk, push-up, and other exercises included in the manuscript contents are examples of circuit training Both types of exercise were shown to significantly increase CK levels (Beiter et al., 2025) [21] Randomized controlled trials Eighteen triathletes 32-33 years Exercise Program A one-hour running session on a motorized treadmill (Saturn, h/p/cosmos) was the workout test. After a 10-minute warm-up at the starting pace needed to run at 75% of the individual anaerobic threshold, the activity progressed to a 50-minute main exercise at a steady pace that corresponded to 90% of the individual anaerobic threshold. Normal ambient temperature (18–21°C, N) was used for the first workout test. After 7–14 days, the second training session was conducted in a moderately hot atmosphere with a temperature of 28-30°C There was a significant increase in CK levels in both groups after the exercise intervention both at normal and at high temperature (Kusmierczyk et al., 2024) [22] Randomized controlled trials Twenty-seven participants 19-25 years Exercise Program The treadmill was used for the downhill running exercise, which was started at a speed of 6 km/h on a -10% slope. Participants' speed was modified to reach 60% of their precisely recorded VO2max after four minutes. Cardiorespiratory parameters were continuously assessed for an hour while this speed was maintained There was a significant increase in CK levels after the intervention (Arriel et al., 2018) [23] Randomized controlled trials 28 trained cyclists 25-28 years Exercise Program The maximal incremental cycling test (MICT) Cyclists carried out one of the four interventions listed below right after the MICT: Two 5-minute occlusion/5-minute reperfusion episodes (PEIC or SHAM, 2 x 5) or five 2-minute occlusion/2-minute reperfusion sessions (PEIC or SHAM, 5 x 2) are other options. Unilateral treatments of SHAM (20 mmHg) or PEIC (50 mmHg above systolic blood pressure) were administered to alternate thighs. A second MICT was conducted 24 hours following There was a significant increase in CK levels after the interventionTable. Summary of the design and intervention of the studies ↓
an isokinetic dynamometer
and eccentric knee flexion exercises, to train the quadriceps and the muscles
of the lower extremities.
exercise's intensity:
10 sets of 12 repetitions,
with a 30-second rest period, for a total of 120 repetitions.
to 90° knee flexion and 60°/s angular velocity.
to significantly increase creatine kinase levels.
120 eccentric movements as closely as possible using the knee extensor muscles.
of 12 repetitions, with 30 seconds rest between sets.
to perform knee extension briefly for dynamometer measurement, and then reduce gradually to 90° knee flexion (60° total range) at a rate
of 60 degrees/second.
to measure the knee movement flow measured by the dynamometer as soon as possible. Each eccentric action lasted for one day, and was performed by the extension patient for one day
participants
at a moderate intensity.
(in pairs) executed four distinct fast bowling periods. Using line (off- and leg-stump) and length (short-, good-, and full-) variations, one player bowled a series of standard bowls
(in 4-over sequence)
at match intensity.
To prolong the bowling spell and meet the over requirements of each experimental trial, the same
4-over routine was repeated
of training were done before the marathon.
was conducted
on the research sample.
the intervention
This study's goal was to ascertain the impact of physical exercise in increasing CK levels after intervention. The results proved that CK levels increased significantly after doing physical exercise. The results of previous studies prove that eccentric workout utilizing an isokinetic dynamometer that involves eccentric knee flexion movements, exercise intensity of a total of 120 repetitions in 10 sets of 12, 30 seconds rest interval proved significant in increasing CK levels after intervention [6]. The findings of additional research also support the notion that the research sample given the intervention to perform 120 maximal eccentric movements with the knee extensor muscles in ten sets of twelve repetitions, with a 30-second break between sets proved significant in increasing CK levels after the intervention [16]. So scientifically, eccentric exercise is proven to increase CK levels. However, we must know how the stages of increase occur and what underlies the increase.
Elderly people who had done previous training so that they participated in the Nijmegen march activities, namely walking with moderate intensity by walking 30, 40, 50 km per day carried out for 4 consecutive days, proved to be significant in increasing CK levels after the exercise intervention [17]. Another finding from the bowling club study was that participants finished a fast bowling skills test in which bowlers (in pairs) executed four distinct fast bowling spells. While the other participant engaged in a simulated fielding exercise, one player executed a series of standardized bowls (in four over sequence) at match intensity, incorporating variations of line (off- and leg-stump) and length (short-, good-, and full-). CK levels significantly increased following the intervention, according to the results [18]. Other data proved that 24 weeks of marathon race preparation training, then participants ran a marathon consisting of running a half, 30 km, and full marathon proved that CK levels increased significantly after the intervention [19].
Supporting this evidence, it is also demonstrated that the findings of additional research support the same conclusion, namely that physical activity intervention raises CK levels [20]. The results of another study conducted on participants with an exercise test intervention for 1 hour on a treadmill and in addition the researchers also compared the effect of temperature on increasing CK levels. The results proved that both the occurrence of temperature differences between cold and hot temperatures after physical exercise interventions proved significant in increasing CK levels [21]. In a different study, participants were given a treadmill with a downhill running exercise intervention on a -10% slope. The participants' initial speed was set at 6 km/h, and after 4 minutes, it was changed to reach 60% of their VO2max, which was precisely measured and maintained for the duration of the intervention. The findings demonstrated that following the physical exercise intervention, CK levels increased [22]. CK levels also increased after the study sample performed the maximal incremental cycling test [23]. So from the results of the review of several studies that have been compiled in this systematic review, all data show the occurrence of CK levels significantly after performing physical exercise interventions. However, it is known to have increased and we must also know the mechanism underlying the increase in CK levels after physical exercise intervention. Therefore, the following discussion will explore in depth how the physiological mechanisms underlying the increase in CK levels after physical exercise.
Physiological mechanisms of physical exercise in increasing creatine kinase levels
Because it is an enzyme of energy and phosphate metabolism involved in the rapid supply and storage of energy, creatine kinase, an intracellular dimeric or octameric protein, is found in body tissues with high energy consumption [24]. One important modulator of cellular energy homeostasis is creatine kinase (CK). CK creates a sizable pool of quickly diffusing phosphocreatine through the reversible interconversion of creatine to phosphocreatine, which buffers ATP levels in the body both geographically and temporally. Therefore, particularly during activity, CK is essential for tissues like muscle and the brain that have high and changing energy demands [24]. This enzyme, which belongs to the phosphoryl transferase family, makes sure that a phosphoryl group is transferred from creatine phosphate to adenosine diphosphate in a reversible manner, creating adenosine triphosphate [25]. In regular laboratory diagnostics, CK has become an essential diagnostic marker because of its subcellular location and variety of functions [26]. In trauma, oxygen deprivation or muscle exhaustion cell homeostasis is upset cause cell damage and cell membranes become leaky. Intracellular components like CK seep out when the membrane ruptures. The subsequent increase in total CK concentration, which can be measured in blood serum, is caused by the sum of all CK isoenzyme fractions, which are primarily supplied by the skeletal muscle isoenzyme fraction. This may be several times higher than typical levels [12].
A substantial intracellular phosphocreatine pool that prevents a precipitous decline in the global ATP concentration and acts as an efficient temporal energy buffer, is formed in part by isoenzymes. The idea of CK isoenzyme subcellular compartmentation and the restricted free passage of even smaller molecules within the cell, like adenine nucleotides, serve as the foundation for additional CK functions [27]. Despite their partial solubility, CK isoenzymes do exhibit some degree of subcellular structural interaction. Metabolite channeling, also referred to as functional coupling, is the process by which CK is directly or indirectly associated with processes that supply or consume ATP, forming microcompartments that often allow direct ADP and ATP exchange between association partners without combining with the bulk solution [28].
For maximum ATP, the local ATP/ADP ratio around the cellular ATPase should be kept high; for oxidative phosphorylation the mitochondrial matrix should have a relatively low ATP/ADP ratio that is possible by the differential microcompartmentalization of CK isoenzymes. According to some theories, CK reactions serve as a kind of intracellular spatial energy transport that makes it easier for high-energy phosphate to move from the mitochondria, which produce ATP, to the cytosol, which uses it, and for the product to return to the mitochondria for rephosphorylation [29]. The CK/phosphocreatine system may theoretically offer the exact localization of mitochondrial and cytosolic isoenzymes, as well as the somewhat quicker diffusion rate of phosphocreatine in comparison to ATP, that results in a spatial "energy shuttle" or "energy circuit," linking the locations of energy generation and consumption [24]. At least in polar and large cells, there is growing evidence that CK and creatine microcompartments and a CK/phosphocreatine shuttle exist, even though some of these roles are still up for debate. Excessive activity in adults raises serum CK levels because it stresses muscle cells, according to studies [30]. Following an intramuscular injection, surgery, electromyography, or biopsy, it may also rise noticeably. Furthermore, CK levels in healthy people exhibit notable physiologic diversity depending on age, sex, and ethnicity, according to other studies [31]. CK increases drastically in skeletal muscle tissue experiencing high energy expenditure [25]. When exercising, it is known that CK levels increase significantly [17]. In addition, increased CK levels are also a sign of muscle damage.
Protein synthesis and degradation interact in a complicated and protracted way as a result of a series of events started by damaged muscle cells [32]. Therefore, muscle atrophy, muscle degeneration, and exercise-induced muscle damage (EIMD) can be caused by the breakdown of proteins [33]. Exercise-induced muscle injury results in altered protein structure, diminished muscular strength, and compromised muscle function. Increased serum levels of skeletal muscle enzymes (lactate dehydrogenase (LDH), myoglobin (Mb), and creatine kinase (CK), as well as decreased force output and neuromuscular deficiencies, are linked to exercise-induced muscle injury [34]. This muscle injury causes EIMD, which is manifested as limb edema, diminished neuromuscular function, and decreased range of motion [34]. These symptoms impair muscular function and make it difficult for athletes to engage in high-intensity training in the days that follow [35]. So maintaining training performance is very necessary, even additional nutrition is very important to maintain physical performance, so that it can be optimal in subsequent training.
Serum creatine kinase and lactate dehydrogenase are indicators of how well the skeletal muscles have adapted metabolically to physical exertion [36]. Serum levels of these enzymes that play a role in the metabolism of muscles, are typically quite low. These enzymes rise dramatically after severe exercise. After intense exercise, both athletes and healthy people have been shown to exhibit changes in blood muscle enzyme activity. Pyruvate is converted to lactic acid during exercise by the enzyme lactate dehydrogenase because active muscles utilize up available oxygen [37]. About 40% of the lactate in the blood is released by skeletal muscle, and the majority of this is subsequently taken up by the kidneys and liver, where it is converted to glucose by oxidation [38]. The muscle enzyme creatine kinase controls the conversion of creatine to phosphocreatine, which is then utilized to produce intracellular adenosine triphosphate [39]. However, during intense anaerobic exercise, creatine supplementation may boost ATP capacity and energy generation, potentially enhancing muscle strength, repetitions, and training volume. These factors may further enhance performance and muscle growth during the training period [40]. In addition, there is an interesting phenomenon of the relationship between CK and catalase (CAT), one of the endogenous antioxidants, during exercise.
CAT depletion happens first during exercise, reflecting rapid consumption to neutralize exercise-induced reactive oxygen species (ROS), whereas CK increases later, peaking after exercise as sarcolemmal damage from cumulative oxidative stress, mechanical tension, and ROS-induced inflammation allows the enzyme to leak into the bloodstream [41]. This temporal dissociation highlights the direct threat to membrane integrity posed by CAT's incapacity to fully counteract oxidative stress. This exacerbates CK release through mitochondrial dysfunction, lipid peroxidation, and protease activation, all of which contribute to the breakdown of muscle structure [42]. Consequently, CK is a delayed signal of permanent damage, but CAT is an early indicator of oxidative imbalance. This leads to a feedback loop in which unresolved oxidative stress (represented by prolonged suppression of CAT) exacerbates mechanical injury (represented by persistently high CK) [43]. As of right now, the rise in CK levels during exercise is a physiological reaction that aims to produce more ATP. To move other organs and perform skeletal muscle activity, the body needs to produce more ATP in order to achieve homeostasis.
Strenght and limitations
This systematic review's advantage is that it just examines randomized controlled trials, which eliminates the chance of unclear cause-and-effect linkages and being the most trustworthy form of scientific data. Furthermore, the samples collected are human-focused, exhibit consistent data, and aren't combined with samples from other categories, like animal samples.
We realize the limitations of this systematic review, we only focus on conducting an in-depth analysis of how exercise affects increased creatine kinase levels. In discussing physiological responses and their mechanisms, it may be felt to be less in-depth, but that is the limitation of researchers because they are aware of the complexity of physiological mechanisms that occur in the body. To examine it in other biomarkers such as how the stages of creatine kinase occur during physical exercise, experimental research is needed. In addition, a comparison between high and low intensity exercise also needs to be studied in depth, therefore further research is recommended to solve this problem.
CONCLUSIONS
Contributors:
Putro B.N. – data curation, visualization;
Wibawa J.C. – conceptualization, writing, original draft;
Ayubi N. – conceptualization, original draft.
Acknowledgement
We would like to express our gratitude that this publication has received funding from Universitas Sebelas Maret.
Funding. This research received no external funding.
Conflict of interests. The authors declare no conflict of interest.
REFERENCES
 UK
UK  EN
EN